creation date: 2026-04-05 23:54
tags: Pathologies
Disseminated Intravascular Coagulation
Background
Definitions
Disseminated intravascular coagulation (DIC) is a condition of disrupted hemostasis, wherein systemic activation of the coagulation processes result in the formation of microthrombi in small vessels throughout the body.
If not promptly identified and treated, organ dysfunction and depletion of clotting factors resulting in uncontrolled bleeding will occur.
Etiology
DIC is a secondary manifestation of underlying conditions.
Pregnancy-related causes:
- Placental abruption (37%)
- Postpartum hemorrhage (29%)
- Preeclampsia/eclampsia/HELLP syndrome (14%)
- Acute fatty liver of pregnancy (8%)
- Amniotic fluid embolism (6%)
- Pregnancy-related sepsis (eg. septic abortion, severe chorioamnionitis, portpartum endometritis) (6%)
Nonpregnancy-related causes:
- Sepsis
- Trauma
- Cancer
Pathogenesis
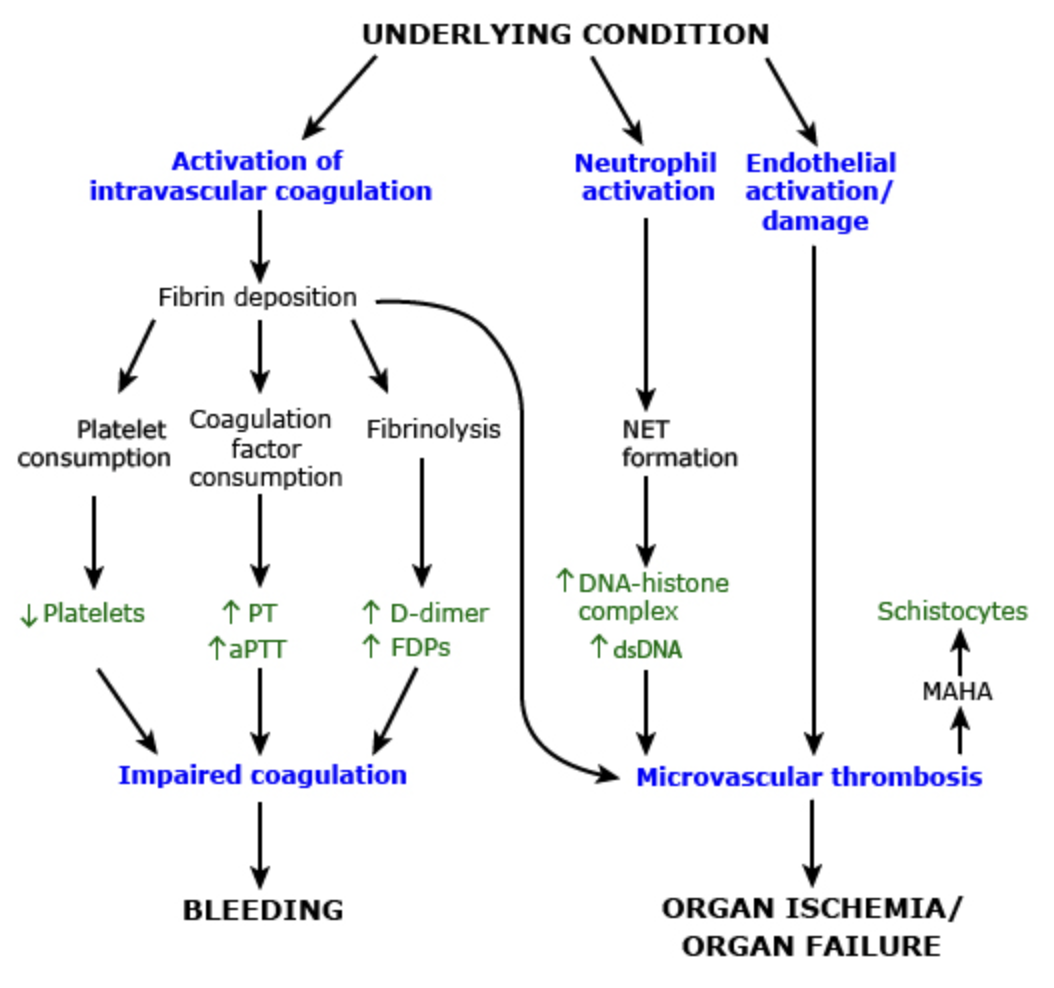
DIC is characterized by abnormal activation of both coagulation and fibrinolysis resulting in ongoing systemic clot formation and subsequent breakdown.
Typical sequence of pathogenesis is as follows:
- Blood is exposed to normally protected procoagulants (eg. tissue factor)
- Coagulation cascade is activated causing formation of thrombi, consuming coagulation factors and platelets
- Fibrinolysis is activated at sites of thrombus formation
- Compensation occurs (synthesis of coagulation factors and platelets)
Compensation may be adequate or inadequate (often referred to as chronic and acute DIC, respectively). As thrombosis, reduced perfusion, and/or bleeding occurs, tissue or organ damage may result.
Clinical Presentation
Signs & Symptoms
Presentation varies based on the underlying etiology and severity.
Overt DIC
Overt fulminant DIC is more common in pregnancy as coagulation and fibrinolysis are both increased.
Overt bleeding and thrombosis are present:
- Severe vaginal bleeding (note that concealed abruption is possible)
- Diffuse oozing from skin (eg. at IV sites) or mucosa (eg. bladder catheter)
- Signs of shock
- Organ dysfunction (AKI, hepatic dysfunction, lung injury, neurologic dysfunction)
Latent and compensated activation of coagulation
Presents without obvious clinical symptoms and is often a chronic conditions.
- Subtle hemostatic dysfunction
- Increased thrombotic risk
History & Physical Exam
If unknown, a prenatal history of complications should be obtained.
If not pregnant or a non-pregnancy associated etiology is suspected, inquire about:
- Cancer history
- Trauma
- Infection and possible source of sepsis
Risk Factors
Primary risk factor is the presence of pregnancy complication.
Diagnosis
Criteria
Diagnosis is made with a combination of clinical setting (eg. in pregnant patient with complication) and laboratory evidence of:
- Thrombocytopenia
- Coagulation factor consumption
- Fibrinolysis (d-dimer)
Work-up
Initial laboratory workup
- CBC (thrombocytopenia)
- Coagulation studies (prolonged aPTT, PT, and TT)
- Fibrinogen level (decreased)
- D-dimer (elevated)
- Liver function tests (normal with DIC; abnormal suggests liver pathology)
- Thromboelastography (TEG)/rotational thromboelastometry (ROTEM)
- BUN and creatinine (elevated with AKI)
- Cultures if sepsis is suspected
Differential
Other causes of bleeding, especially around pregnancy, include:
- Postpartum hemorrhage with dilutional coagulopathy
- Primary thrombotic microangiopathy (eg. TTP)
- von Willebrand disease
Other conditions in the setting of shock and elevated d-dimer include:
- Pulmonary embolism
- Antiphospholipid syndrome
Red Flags / Complications
Management
Treatment of Underlying Cause and Supportive Measures
Treatment consist of management of underlying cause to eliminate stimulus for ongoing coagulation and thrombosis.
Additional supportive measures may be used:
- Hemodynamic and/or ventilatory support
- Aggressive hydration of acute hemolytic transfusion reaction
- Blood product transfusion for severe bleeding
Systemic Therapies
Generally, systemic therapies are not used routinely.
Prevention/treatment of bleeding
Prophylactic administration of platelet and coagulation factors may be considered if patient is at high risk of bleeding and/or if platelet count is <10,000/mcL.
Patients who are bleeding or may be at risk (eg. surgery) with platelets <50,000/mcL should be given platelets:
- 2 units/10 kg body weight
Patients with serious bleed and significantly prolonged PT, aPTT, or decreased fibrinogen should receive coagulation factor replacement:
- Fresh Frozen Plasma (FFP)
- Cyroprecipitate
Other considerations
Antifibrinolytic agents (eg. TXA, EACA, aprotinin) are contraindicated due to risk of thrombotic complications.
Prophylactic anticoagulation for thrombosis risk is also not indicated. Anticoagulation may be considered in the context of VTE treatment.