creation date: 2025-07-09 01:48
tags: Workups
Abdominal Pain
Background
Abdominal pain is both common and diverse in causes. In most cases, abdominal pain is benign and/or self limiting but it is important to evaluate for serious etiologies.
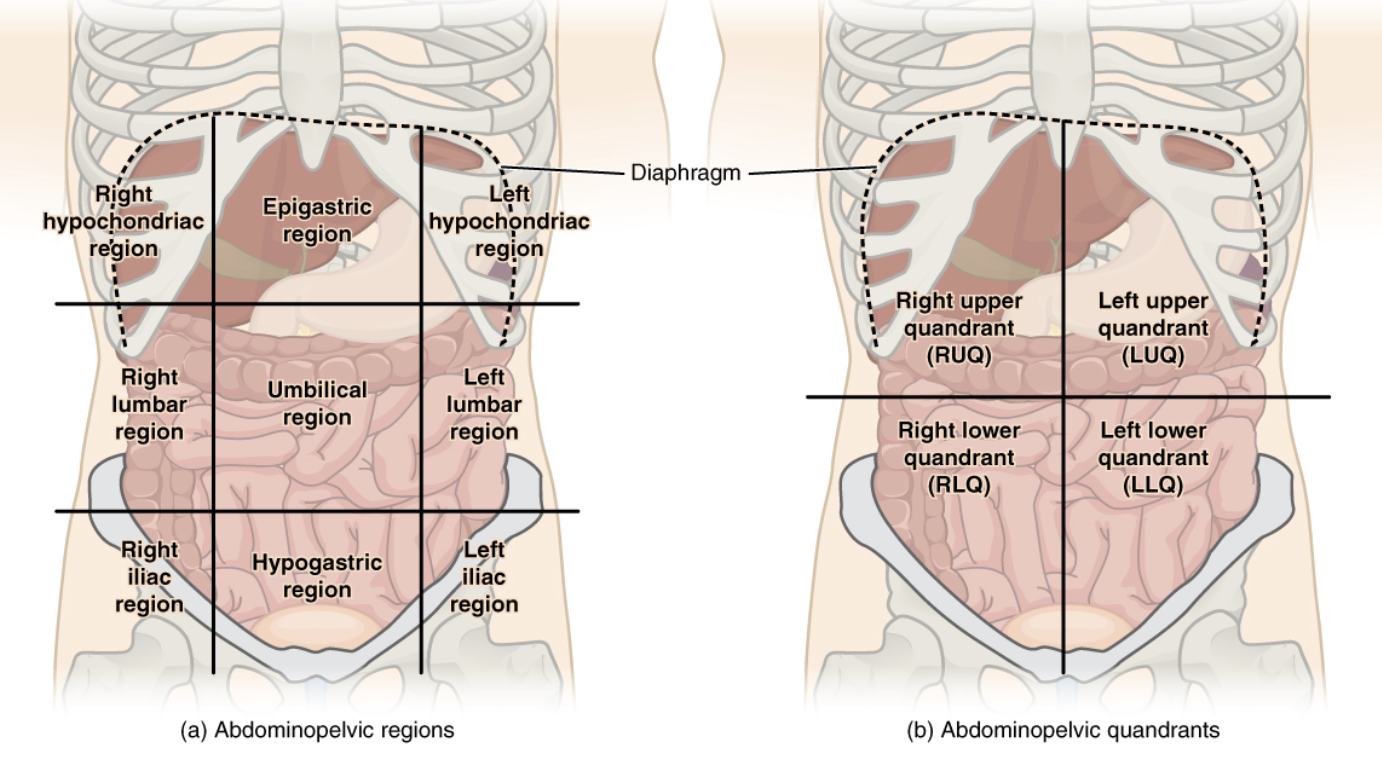
The abdomen is divided for ease of communication. This is either into 4 quadrants or into 9 regions.
Pathophysiology
The perception of pain originates from pain receptors in the abdomen which response to mechanical and chemical stimuli.
Visceral nociceptors: mechanical stimuli is primarily stretch but will respond to distension, contraction, traction, compression, and torsion. Can also detect chemical stimuli.
Visceral mucosal receptors: primarily respond to chemical stimuli.
Pain is generally midline for digestive tract pain due to symmetric bilateral innervation while lateralized pain may suggest ipsilateral structures (eg. kidney, ovary).
Referred pain may also occur with the associated dermatome entering the spinal cord at the same position (eg. gallbladder pain perceived in scapula)
Differential Diagnosis
Upper Abdomen
Right Upper Quadrant
- Cholelithiasis (gallstones)
- Cholecystitis
- Ascending Cholangitis
- Sphincter of Oddi dysfunction
- Hepatitis
- Perihepatitis
- Liver abscess
- Budd-Chiari syndrome (hepatic venous outflow tract obstruction)
- Portal vein thrombosis
Epigastric
- Myocardial infarction
- Pancreatitis
- Peptic ulcer disease
- Gastroesophageal reflux disease
- Gastritis/gastropathy
- Functional dyspepsia
- Gastroparesis
Left Upper Quadrant
- Splenomegaly
- Splenic infarction
- Splenic abscess
- Splenic rupture
Lower Abdomen
Right Lower Quadrant
- Acute appendicitis (periumbilical that radiates RLQ)
- Diverticulitis (less common)
Left Lower Quadrant - Diverticulitis (more common)
**Unilateral but can be either side - Kidney stones
- Pyelonephritis
Suprapubic or not localized to side - Cystitis (Uncomplicated UTI)
- Acute urinary retention
- Infectious colitis
Diffuse or Nonspecific Abdominal Pain
- Obstruction (eg. small bowel obstruction, colorectal cancer, gastric volvulus)
- Perforation of GI tract
- Mesenteric ischemia
- Inflammatory bowel disease (eg. ulcerative colitis and Crohn disease)
- Viral gastroenteritis
- Spontaneous bacterial peritonitis
- Peritonitis due to peritoneal dialysis
- Malignancy (eg. colorectal cancer, gastric cancer, pancreatic cancer)
- Celiac disease
- Ketoacidosis
- Adrenal insufficiency
- Foodborne disease
- Irritable bowel syndrome
- Constipation
- Diverticulosis
- Lactose intolerance
Other less common causes
- Abdominal aortic aneurysm
- Abdominal compartment syndrome
- Abdominal migraine
- and more
Initial Evaluation
History
Detailed history is generally insensitive and nonspecific, especially for benign conditions but more effective for elucidating more serious causes.
Onset (acute vs. chronic):
- New problem or long standing issue
- Possible that patient has chronic condition that is exacerbating or new, unrelated issue overlapping
Provoking or palliation: - Worsening or onset with eating
- Occurring with specific food types (eg. lactose or gluten)
- Pain with motion (eg. peritonitis)
Quality: - Burning or gnawing (GERD or peptic ulcer disease)
- Colicky/cramping (eg. gastroenteritis)
Radiation: - Location of pain and where it radiate is often characteristic for specific etiology
Severity: - Pain severity generally correlates with severity of condition
- Be aware of corticosteroids or other pain medication that can modify the pain level
Time: - Gradual and steady may suggest something like pancreatitis
- Maximal and sudden onset might suggest something like perforation
Associated symptoms can provide much more information on the etiology:
- Other GI symptoms such as:
- Nausea and/or vomiting
- Diarrhea or constipation
- Hematochezia/BRBPR
- Melena
- Changes in stool
- Liver disease related symptoms:
- Jaundice
- Changes in urine and/or stool colour
- Genitourinary symptoms:
- Dysuria
- Frequency
- Hematuria
- Constitutional symptoms (suggests infection, malignancy etc.):
- Fevers
- Chills
- Fatigue
- Weight loss
- Anorexia
- Cardiopulmonary symptoms:
- Cough and/or shortness of breath
- Orthopnea
- Exertional dyspnea
- Condition specific symptoms:
- DKA may present with polyuria and thirst
Consider a sexual history if there are suspicion of STDs and/or pelvic inflammatory disease. For women, questions regarding menstrual history and vaginal symptoms may be warranted.
Past medical history including surgeries should be obtained. Abdominal surgery is a risk factor for adhesion and thus obstruction. Cardiovascular disease may raise concerns for cardiac etiology.
Medication history is also relevant such as chronic and/or high-dose NSAID use is a risk factor for a number of conditions.
Other components of the history include:
- Alcohol use
- Family history
- Travel history
- Sick contacts
Physical Exam
Objective exam should consist of at least vitals and abdominal exam.
In cases of suspected fecal impactation, a rectal exam should be done. Consider a pelvic exam if pelvic pathology is considered.
Investigations
Further studies are determined by the history and physical and based on the suspected etiology.
In settings where possible (eg. emergency department), a point-of-care ultrasound can be done.
Laboratory tests are typically routinely ordered unless an etiology is already established:
- Pregnancy test (hCG)
- CBC
- Electrolytes
- Serum lactate and venous blood gas
- Liver and pancreatic enzymes
- Coagulation studies and blood types - if gastrointestinal bleed
- ESR and CRP - for inflammatory and infectious processes
- Urinalysis - for suspected GU etiology
- D-dimer - for vascular occlusive diseases
- STI testing - if suspected
Chest radiograph can be considered if cardiothoracic symptoms present and ECG if suspicion of ACS. In patients with ascites, an abdominal paracentesis may be done and ascitic fluid analyzed for certain etiologies.
In cases of still undifferentiated abdominal pain, a CT abdomen is often diagnostic. Use of IV contrast improves diagnostic accuracy but may cause acute kidney injury (primarily those with eGFR <30).
Abdominal radiographs are generally low yield and thus not routine.