creation date: 2025-07-03 00:26
tags: Pathologies
Cholelithiasis
Background
Definitions
Cholelithiasis or cholecystolithiasis refers to the presence of gallstones in the gallbladder.
Gallstones are made up primarily of cholesterol but can be pigmented depending on composition.
Note, gallstones within the common bile duct (choledocholithiasis) is discussed separately.
Etiology and Pathogenesis
Formation
In normal physiology, primary bile acids are formed from cholesterol in the liver mediated by vitamin C and are soluble.
Gallstones are formed from bile products that precipitate out of the solution including:
- Cholesterol
- Products from the breakdown of red blood cells
- Mixture of calcium bilirubinate, phosphate, carbonate, palmitate, and cholesterol
as well as substances such as postaglandins and lecithin which promote crystallization.
Biliary stasis is a key contributor in gallstone formation. Some causes of impaired gallbladder emptying include:
- Bowel rest
- Prolonged total parenteral nutrition
- Pregnancy
Cholesterol stones
An increase in cholesterol concentration in bile and decrease in bile salts and lecithin results in hypersaturated bile that precipitates as cholesterol and calcium carbonate. These make up 70% of stones.
Risk factors include:
- Obesity, insulin resistance, dyslipidemia
- Female sex (estrogen causes bile rich in cholesterol, progesterone relaxes smooth muscle and can cause bile stasis)
- Multiparity or pregnancy
- Family history
- Drugs: fibrates, estrogen therapy, OCPs
- Malabsorption
- Rapid weight loss
Black pigment stones
Black pigmentation is due to increased hemolysis causing increased in conjugated bilirubin formation. This overwhelms the conjugation process which results in an increase in unconjugated bilirubin that can precipitate. Bilirubin precipitation results in black colouring of stones.
Risk factors include:
- Chronic hemolytic anemia
- Alcoholic cirrhosis
- Crohn disease
- Total parenteral nutrition
- Advanced age
Mixed pigment stones
Mixed or brown stones are due to infection or infestation causing damage to hepatocytes and the subsequent release of ß-glucuronidase which hydrolyzes conjugated bilirubin. Unconjugated bilirubin and fatty acids in bile precipitate as calcium carbonate, cholesterol, and calcium bilirubinate which is dark in colour.
Risk factors include:
- Bacterial infections and parasites in the biliary tract
- Sclerosing cholangitis
Clinical Presentation
Signs & Symptoms
Most gallstones are asymptomatic with many found incidentally.
In symptomatic cases, gallstones may present as biliary colic:
- Constant, dull RUQ pain lasting < 6 hours
- Often coincides postprandial
- Pain may radiate to epigastrium, right shoulder, and back (referred pain)
Other non-specific symptoms include:
- Nausea and vomiting
- Early satiety
- Bloating and dyspepsia
Note that complications can be the first manifestation of gallstones.
History & Physical Exam
History should elicit details regarding any pain felt. Pain that lasts longer than the 6 hours suggesting biliary colic should raise suspicion for more concerning conditions such as cholecystitis or choledocholithiasis.
Physical exam may note abdominal tenderness during biliary colic but would otherwise be unremarkable. Complications may present with more severe findings.
Risk factors
Discussed in Etiology and Pathogenesis as risk factors vary based on composition.
Diagnosis
Criteria
Diagnosis is made using imaging which includes incidental findings.
In patients with suspected symptomatic cholelithiasis, ultrasound is the preferred modality (whether POCUS or transabdominal RUQ ultrasound).
Ultrasound findings
Characteristic findings for gallstones:
- Intraluminal highly echogenic foci
- Strong posterior acoustic shadowing
- Rolling stone sign: movement of echogenic foci with patient movement
and biliary sludge:
- Low-level echogenic material in dependent portion of gallbladder
- No posterior acoustic shadowing
- Slow movement with changing of patient position
Gallbladder calculi and wall thickening:
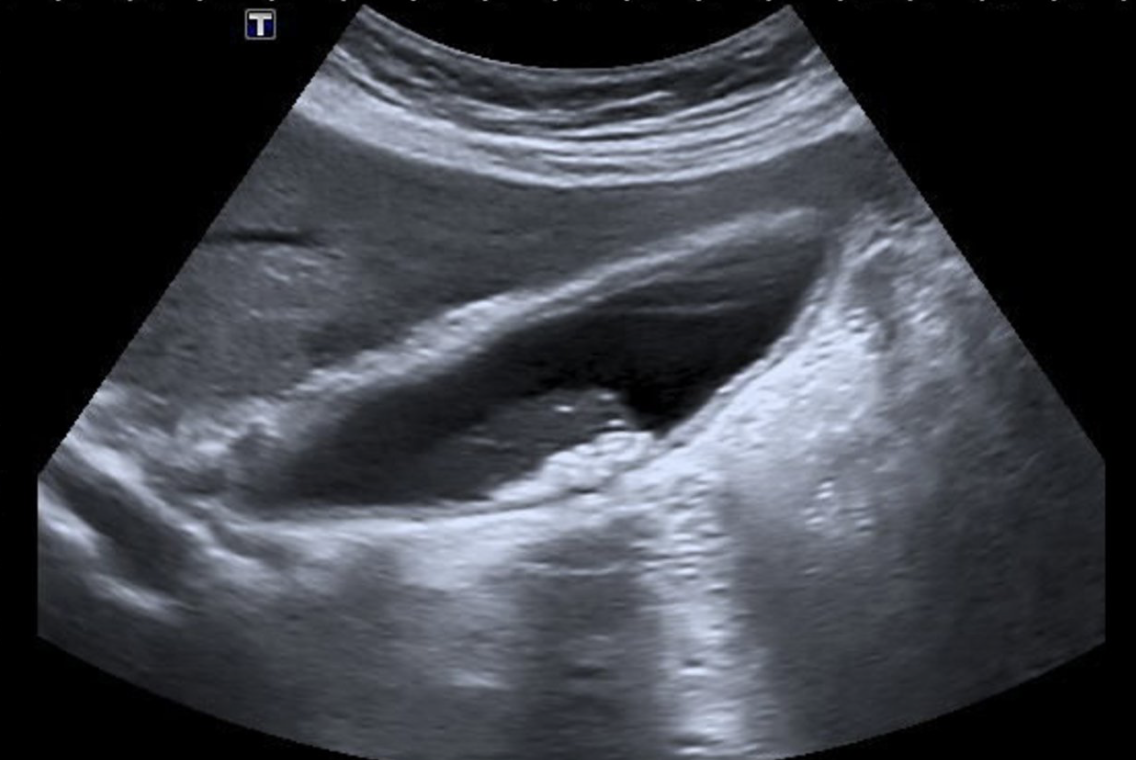
Cholelithiasis:

Work-up
Beyond imaging, workup includes ruling out complications.
- Dilation of common bile duct may suggest Choledocholithiasis and would require additional workup
- Gallbladder wall thickening and/or pericholecystic fluid may suggest acute cholecystitis
Laboratory studies are typically normal but used to rule out additional conditions and other causes of acute abdominal pain.
- Complete blood count
- Liver function tests
- Amylase and lipase
In cases of inconclusive findings or suspected choledocholithiasis, consider MRI abdomen with and without IV contrast with MRCP.
- Well-defined hypointense (T2) filling defects in gallbladder lumen
If MRI not available or there are suspected complications or alternative diagnoses, CT abdomen with IV contrast can be used.
- Radiopaque stones seen as hyperdense foci in gallbladder lumen
- Note, non-radiopaque stones (eg. cholesterol stones) may not be detected
Differential
Diagnoses with abdominal pain can be varied and discussed separately in its own workup.
A number of other conditions are related to gallstones or the gallbladder which may present similarly.
- Acute cholecystitis - more severe and unrelenting pain, mass may be palpated in RUQ due to edematous and thickened gallbladder. May also have fever and/or tachycardia
- Common bile duct obstruction - jaundice is common and more epigastric pain if pancreas is affected
- Ascending Cholangitis
Red Flags / Complications
Gallstones can impede gallbladder motility and result in inflammation:
- Acute or chronic cholecystitis
- Porcelain gallbladder
- Empyema
- Gangrenous cholecystitis
- Emphysematous cholecystitis
Obstructions within the common bile duct can lead to:
- Jaundice
- Proximal dilation of biliary tree
- Pancreatitis
- Cholangitis
Stones can also compress a duct (Mirizzi syndrome) or become impacted, erode the wall, and form a cholecystoenteric fistula (Bouveret syndrome).
Management
In asymptomatic patients, management is largely expectant with instructions for a return to clinic/emergency room with symptom onset. Prophylactic cholecystectomy can be considered.
In symptomatic, uncomplicated cholelithiasis, initial therapy are supportive:
- Bowel rest until pain subsides (NPO)
- Analgesics such as NSAIDs or opioids if pain does not improve with NSAIDs
- Spasmolytics may be used with analgesics in severe pain
- IV fluids and antiemetics may be used for protracted vomiting
Lifestyle modifications are also used for prevention of recurrence:
- Low-fat diet (especially saturated fats)
- Avoid lithogenic drugs (eg. estrogen, fibrates)
- Regular exercise
Other therapies may be considered such as oral bile acid dissolution therapy and extracorporeal shock wave lithotripsy (ESWL) but they often have high rates of recurrence.
Consider surgical consult if pain is intractable.
In symptomatic, complicated cholelithiasis, management by general surgery and/or gastroenterology is recommended for laparoscopic cholecystectomy to prevent recurrence.