creation date: 2025-11-03 15:51
tags: Pathologies
Pneumothorax
Background
Definitions
Pneumothorax (ptx) is a collection of air outside of the lung within the pleural cavity between the parietal and visceral pleura. The air accumulation can apply pressure on the lung and cause it to collapse.
Pneumothoraces are classified as simple (spontaneous), tension, or open which is discussed below.
Etiology and Risk Factors
Risk factors for primary spontaneous pneumothoraces are:
- Smoking
- Tall thin body habitus in an otherwise healthy person
- Pregnancy
- Marfan syndrome
- Familial pneumothorax
Diseases that may lead to secondary spontaneous pneumothoraces are:
- COPD
- Asthma
- HIV with pneumocystis pneumonia
- Necrotizing pneumonia
- Tuberculosis
- Sarcoidosis
- Cystic fibrosis
- Bronchogenic carcinoma
- Idiopathic pulmonary fibrosis
- Severe ARDS
- Langerhans cell histiocytosis
- Lymphangioleiomyomatosis
- Collagen vascular disease
- Inhalational drug use like cocaine or marijuana
- Thoracic endometriosis
Iatrogenic causes includes biopsies and catheter insertions. Traumatic pneumothoraces result from rib fractures, and penetrating or blunt trauma.
Any of the above etiologies can progress to tension pneumothorax.
Pathogenesis
Air can enter the pleural space by two mechanisms. Traumatic pneumothoraces result from a connection of the interpleural space to the chest wall or to the lung.
Atraumatic pneumothoraces are described as either primary or secondary, which refer to spontaneous pneumothorax without eliciting event and spontaneous pneumothorax occurring after underlying pulmonary disease.
In tension pneumothorax, the positioning of the pleura results in a one-way valve which does not allow for air to escape resulting in a more life-threatening air collection.
Clinical Presentation
Signs & Symptoms
The primary symptoms are:
- Acute dyspnea
- Chest pain (classically pleuritic)
The severity of the symptoms correlates with the volume of air in the pleural space.
Physical findings include:
- Decreased chest excursion on affected side
- Enlarged hemithorax on affected side
- Diminished breath sounds
- Absent tactile or vocal fremitus
- Hyperresonant percussion
With sizeable pneumothorax, laboured breathing and accessory muscle use may be present. Tracheal deviation away from affected side may be seen with tension pneumothorax but may manifest late.
History & Physical Exam
Pneumothorax usually presents with:
- Sudden onset of symptoms
- Unilateral pain (ipsilateral to ptx)
Pneumothoraces can occur in all ages but primary spontaneous cases are typically early 20s, while secondary cases are in patients who are older owing to emphysema.
An assessment of hemodynamic stability should be done as compromise can be an ominous sign of tension pneumothorax and/or impending cardiopulmonary collapse.
An assessment of risk factors should also be made. Physical exam should include cardio and respiratory examination.
Diagnosis
Criteria
Diagnosis of pneumothorax is radiologic. The imaging modality depends on the stability of the patient on presentation and the degree of suspicion.
In unstable patients, bedside ultrasonography is usually used before emergency thoracostomy.
In most cases, pneumothorax can be easily appreciated on chest radiograph. CT can be used when the diagnosis is uncertain.
The classification of pneumothorax can be made based on the following definitions:
- Simple - the mediastinal structures does not shift
- Tension - the mediastinal structures shift
- Open - an opening in the chest wall causes pneumothorax
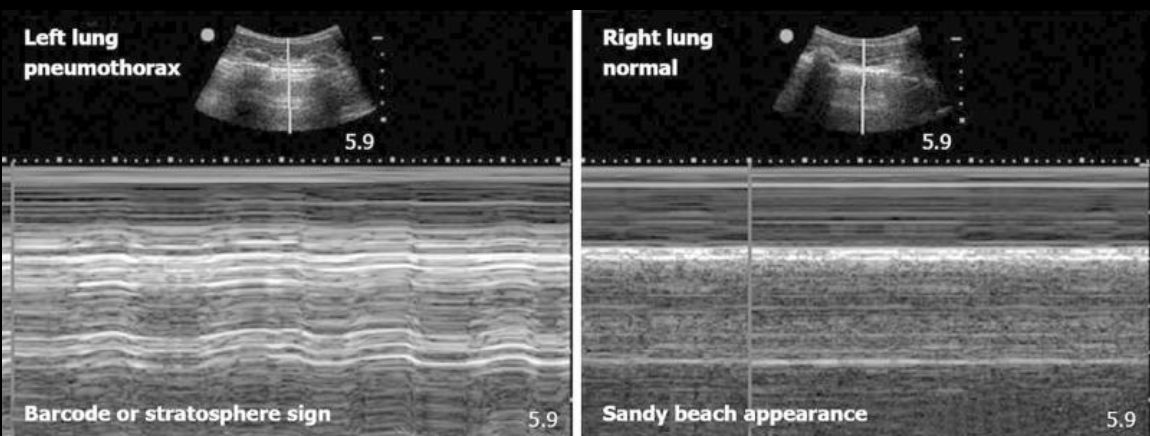
Ultrasound findings
With ultrasound, “M-mode” (motion-mode) is used to visualize the movement of the pleural layers as they slide with respiration.
With pneumothorax, normal lung sliding is not present and thus presents with the barcode sign while the seashore sign is seen in normal lungs:
Chest x-ray findings
Findings on CXR includes:
- Visible visceral pleural edge seen as a thin, sharp white line
- No lung markings peripheral to this line
- Peripheral space is radiolucent compared to adjacent lung
- Lung may fully collapse
- Mediastinum may shift away if tension pneumothorax

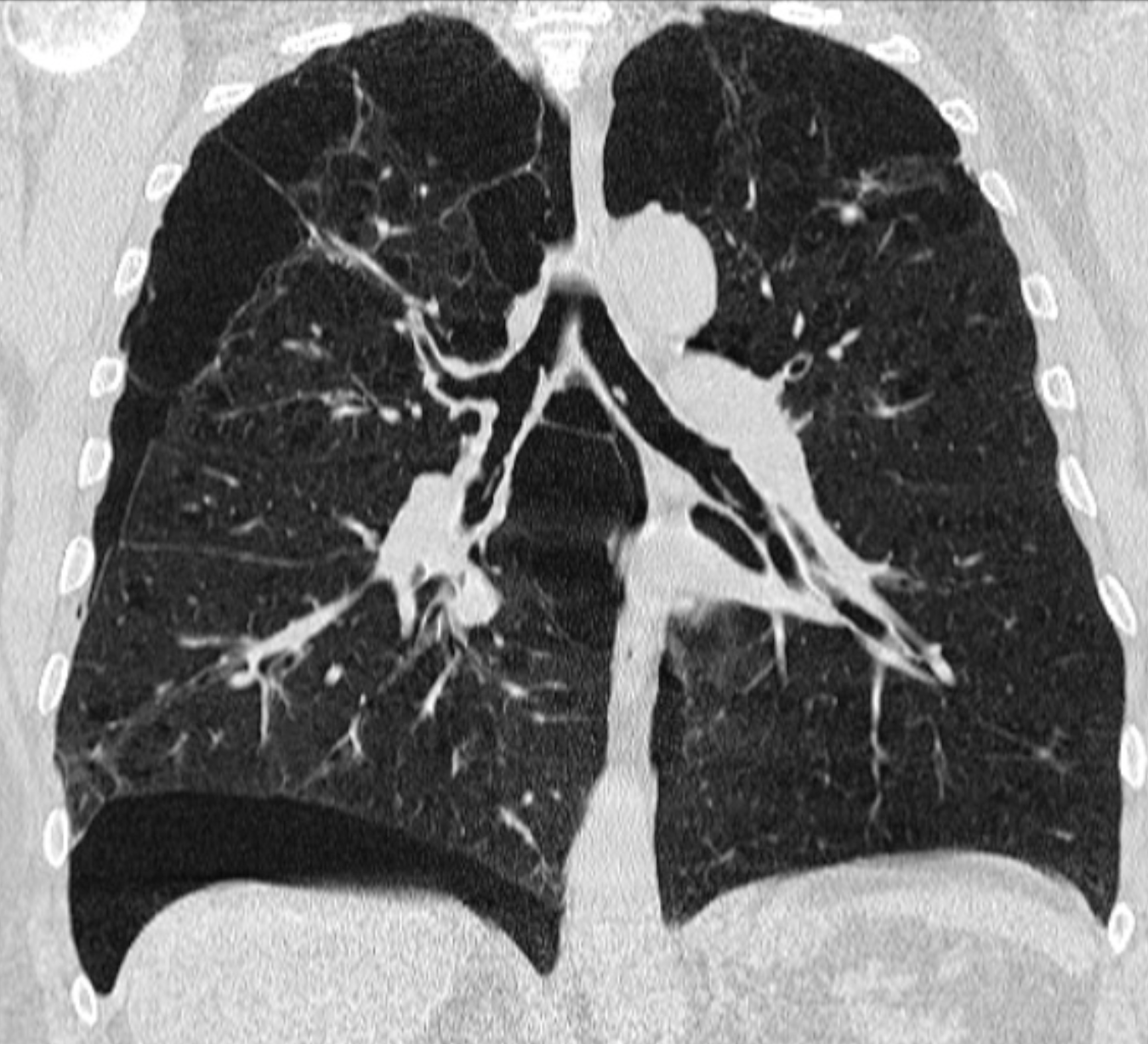
CT findings
Work-up
The importance of the workup centres around identifying potential etiologies inciting the pneumothorax.
In many cases, the etiology may be evident from history and exam. These include trauma or known disorders associated with pneumothorax. In these cases, additional workup is typically unnecessary.
When etiology is not clear, re-evaluation of the imaging and history/physical may be necessary. In some instances, a non-contrast high resolution chest CT may be indicated for etiology. A PFT may also be indicated.
Etiology-specific testing may be performed such as genetic testing for inheritable syndromes (eg. alpha-1 antitrypsin deficiency, Birt-Hogg-Dube, Ehlers Danlos syndrome, Marfan syndrome).
Differential
The differential includes those associated with chest pain.
Other differentials include:
- Pneumonia
- Esophageal spasm
- Rub fracture
- Diaphragmatic injuries
Red Flags / Complications
In large pneumothoraces, there is a risk of death. Tension pneumothoraces is a life-threatening condition.
Management
The treatment of pneumothorax depends on the severity.
Tension pneumothorax
Owing to the urgency of a tension pneumothorax, management consist of:
- Needle decompression (2nd ICS mid-clavicular or 5th ICS mid-axillary)
- Chest tube after
Traumatic pneumothorax
With traumatic pneumothorax, a chest tube is used. Surgery may be indicated if air leak is persistent even with chest tube.
Large or symptomatic primary spontaneous pneumothorax
Needle aspiration is used to remove air (14-16G at 2nd ICS mid-clavicular). If this fails or recurrence occurs immediately, proceed to inserting a chest tube.
Secondary spontaneous pneumothorax
In secondary pneumothorax, patients are admitted (due to high risk of complications) and given supplementary oxygen. If the pneumothorax is too large or if symptoms are present, chest tube is used.
Small, asymptomatic primary spontaneous pneumothorax
If the patient is stable, an observation period with supplementation oxygen may be sufficient. Discharge with follow-up. These cases are typically benign and self-resolving.