creation date: 2024-12-17 11:08
tags: Pathologies
Hypertension
Background
Definitions
High blood pressure or normal blood pressure with treatment.
This page focuses on primary hypertension (formerly essential hypertension).
Etiology
The exact etiology is unclear. However, risk factors are strongly associated with development of hypertension.
Pathogenesis
Arterial blood pressure is the product of the following:
Blood pressure is primarily determined by the sympathetic nervous system, the renin-angiotensin-aldosterone system, and plasma volume (which is controlled primarily by the kidneys). These systems are affected by a number of genetic and environmental factors resulting in hypertension.
Clinical Presentation
Signs & Symptoms
Hypertension is typically asymptomatic until complications arise.
History & Physical Exam
Blood pressure should be assessed at every appropriate office visit. Frequency and timing of screening (incl. using home blood pressure monitor (HBPM)) can be tailored for patient’s risk of hypertension.
Exam should also be done for suspected target organ damage due to complications of hypertension.
Risk factors
- Age - advancing age associated with incidence and systolic BP
- Obesity/weight gain
- Family history - twice as common in patients with hypertensive parents
- Race - tends to be more common, severe, occur earlier in life, and greater organ damage in Black patients
- Reduced nephron number - due to genetics, development, postnatal environment
- High sodium diet (in addition to decreased potassium intake)
- Excessive alcohol consumption
- Physical inactivity
- Insufficient sleep - sleep <7h per night is associated with higher risk of hypertension
- History of gestational hypertension or preeclampsia - even if BP normalized after delivery
- Social determinants
Hypertension may also be secondary which can coexist with risk factors, further complicating treatment. Secondary hypertension can result from a number of conditions.
Diagnosis
Criteria
Diagnosis of hypertension requires ruling out white coat hypertension.
Office visit assessment involves:
- Accurate measurement using recommended technique via AOBPM, OBPM
- Taking an average of at least 3 measurements in the same visit
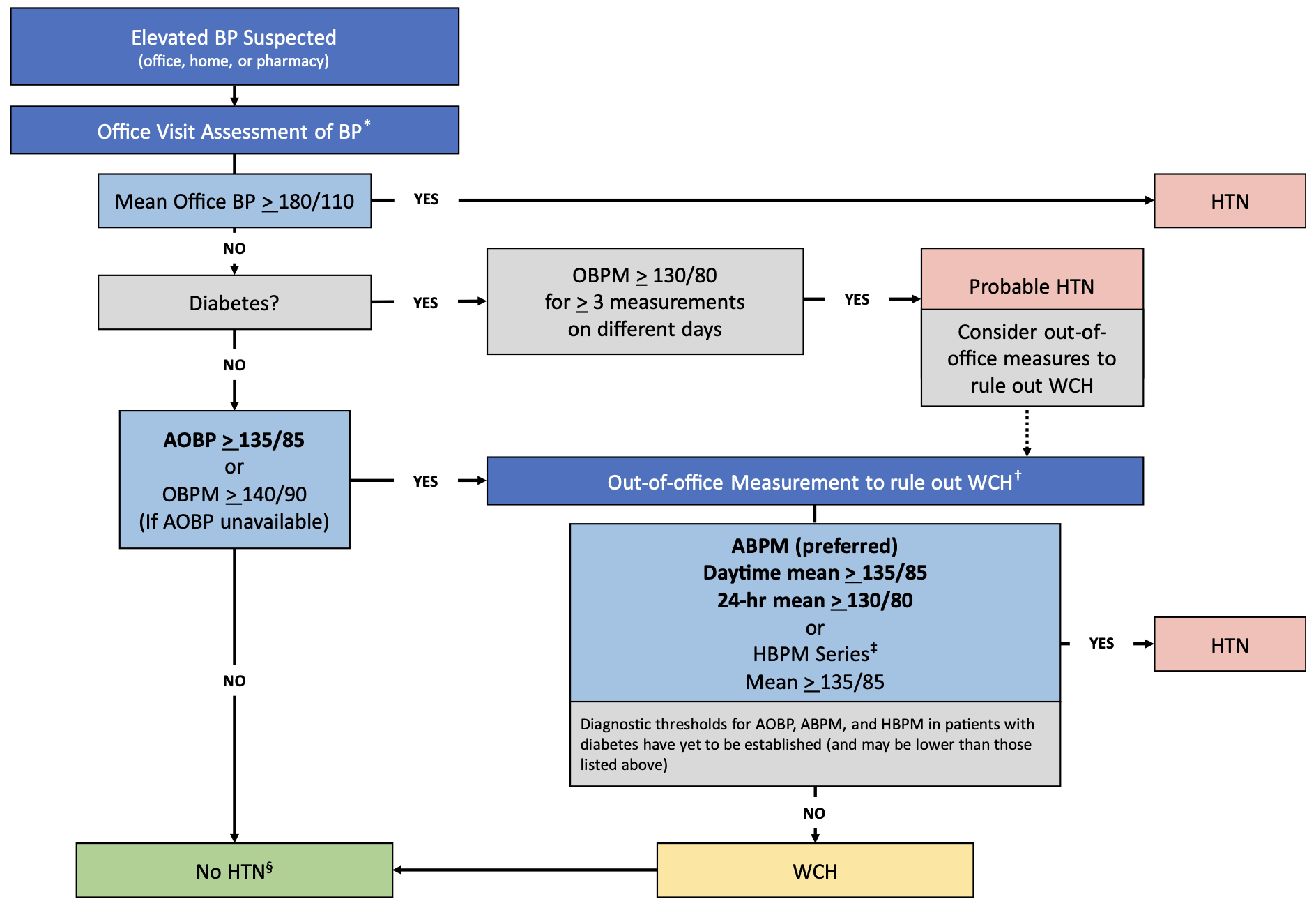
In summary, hypertension is diagnosed with one of the following:
- Office BP ≥180/110
- Office BP ≥130/80 for at least 3 measurements on different days (ruled out WCH)
- Office BP ≥140/90 (rule out WCH)
- Automated office BP ≥135/85 (rule out WCH)
To rule out white coat hypertension:
- Ambulatory BP of ≥135/85 (daytime mean) or ≥130/80 (24h mean)
- Home BP ≥135/85
Hypertensive urgency is defined as DBP ≥130 and asymptomatic.
Hypertensive emergency is defined as DBP ≥130 with target organ damage.
Work-up
Diagnostic work-up requires ruling out white coat hypertension as seen in the above section.
Following a confirmed diagnosis, baseline assessment should be done of the following:
- Cardiovascular risk factors (incl. screening for diabetes, dyslipidemia, and Chronic Kidney Disease)
- Target organ damage
- Routine lab testing
Testing should include:
- Electrolytes including calcium and serum creatinine (for eGFR)
- Fasting glucose
- Urinalysis
- CBC
- TSH
- Lipid panel
- Electrocardiogram
- Calculation of 10 year ASCVD risk
Other tests that may be indicated include:
- Echocardiograph (for LVH)
- Urinary albumin to creatinine ratio (albuminuria is risk factor for CVD)
Testing for secondary hypertension is not routine.
Differential
Unusual presentations, such as onset at a young age or unexpected elevation, may suggest secondary causes. Secondary causes include:
- Renovascular hypertension - most common reversible cause due to decreased blood flow due to atherosclerotic renal artery stenosis causes activation of RAAS
- Primary kidney disease (Acute Kidney Injury or Chronic Kidney Disease) - suggested by elevated serum creatinine and/or abnormal urinalysis
- Primary aldosteronism
- Obstructive sleep apnea
- Medication (incl. OCPs, corticosteroids)
- Illicit drugs (incl. cocaine)
- Pheochromocytoma
- Cushing’s syndrome
- Coarctation of the aorta - typically seen in young children
Red Flags / Complications
Uncontrolled hypertension is associated with significant risk of target organ damage / adverse cardiovascular and renal outcomes. These include:
- Cerebrovascular disease (incl. stroke and Dementia)
- Retinopathy
- Left ventricular hypertrophy and/or congestive heart failure
- Chronic Kidney Disease
- Vascular damage resulting in atherosclerotic changes
- Acute target organ damage such as acute HF, acute coronary syndrome, aortic dissection
Management
Lifestyle / Social
Lifestyle modifications should always be a component of treatment whether alone or with pharmacological therapy. Modifications include:
- Dietary salt restriction
- Potassium supplementation (unless contraindicated by presence of Chronic Kidney Disease)
- Weight loss
- Exercise
- DASH diet (high in vegetables, fruits, low-fat dairy, whole grains, poultry, fish, and nuts; low in sweets, sugar-sweetened beverages, red meats)
- Limit alcohol intake
- Stress management
Patients should also be counselled on HBPM for self-monitoring, especially those with poorly controlled hypertension or comorbidities
Pharmacological / Interventional
Use of antihypertensives are recommended to be strongly considered for SBP ≥140 or DBP ≥90. However, decision to use medication should be individualized, accounting for cardiovascular risk factors.
In adults without compelling indications for specific agents, initial therapy can be either monotherapy of a
- thiazide/thiazide-like diuretic
- beta-blocker
- ACE inhibitor
- ARB
- long acting CCB
or a single-pill combination of - ACE inhibitor or ARB with a CCB
- ACE inhibitor or ARB with a diuretic
Additional antihypertensives can be added if target BP levels are not achieved. Avoid combining ACE inhibitors with ARBs.
Additional considerations should be made if a patient has comorbidities. For example, ACE inhibitors or ARBs are recommended as initial therapy for patients with kidney disease.