creation date: 2025-05-01 18:05
tags: Pathologies
Diabetes Mellitus, Type 2
Background
Definition
Characterized by hyperglycemia, insulin resistance, and relative impairment in insulin secretion. Type 2 diabetes can differ with varying contributions from defective insulin secretion and insulin action/resistance.
Etiology
Development of type 2 diabetes is multifactorial with contributions from
- Genetics - genes relating to beta cell function and insulin action
- Environment - weight gain and decreased physical activity are associated
- Intrauterine development - extremes of birth weight and prematurity
- Drug-induced hyperglycemia - reducing glucose tolerance
Pathogenesis
Pathogenesis of type 2 diabetes can vary in the degree of insulin resistance and defective insulin secretion. Regardless, patients will have a increased demand for insulin mediated by resistance that is not matched by insulin secretion.
Insulin resistance is typically attributed to environmental causes and may be due inflammatory mechanisms. Some other possible mechanisms include:
- Central obesity resulting in increased plasma free fatty acid, which impair glucose uptake
- Increased serine kinase activity causing phosphorylation of IRS-1 and downstream reduction of GLUT4 channels
Insulin secretion dysfunction are suggested to be more dependent on genetics.
Initial insulin resistance is compensated by increased insulin and amylin secretion but as disease progresses, secretion declines while resistance continues to increase.
Normal physiology
Insulin is secreted in the beta-cells of the islet of Langerhans of the pancreas. Insulin (chain A + B) and C-peptide is produced from the cleavage of proinsulin.
Insulin is an anabolic hormone which increases glycogenesis, and decreases glycogenolysis and gluconeogenesis. This results in a decrease in blood glucose levels and counters the effects of hormones such as glucagon, cortisol, catechol, growth hormone, and thyroid hormone.
Insulin also inhibits proteolysis and stimulates protein synthesis, maintains fat stores, and stimulates intracellular potassium accumulation.
Normal blood glucose levels should be:
- 3.8-6.1 mmol/L fasting
- <7.8 mmol/L 2 hrs post-prandial
The range for glucose should stay within 4.0-10.0 mmol/L. Glucose will enter the urine when blood glucose ≥14.0 mmol/L.
Clinical Presentation
Signs & Symptoms
Type 2 diabetes most often present gradually and asymptomatically. Symptoms of complications may be first clinical sign noted.
Classically, hyperglycemia presents with:
- Polyuria
- Polydipsia
- Polyphagia
Other non-specific symptoms may include:
- Unexplained weight loss
- Visual disturbances
- Fatigue
- Pruritus
- Poor wound healing
- Increased susceptibility to infections - results in recurrent infections/inflammations
- Calf cramps/peripheral neuropathy
Insulin resistance can also manifest with cutaneous signs such as:
- Benign acanthosis nigricans (hyperpigmented plaque on neck and axilla)
- Acrochordons (benign skin tags)
History & Physical Exam
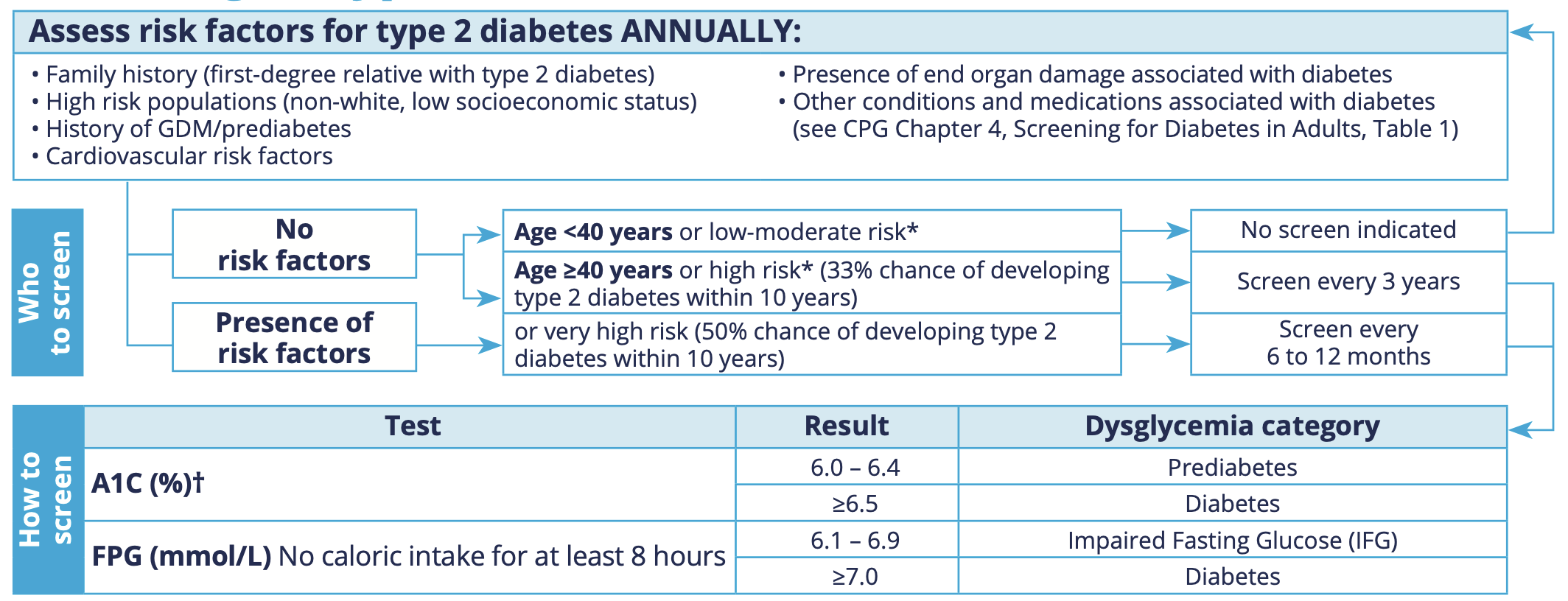
Assessment of risk factors should be done annually for T2DM. Further screening by blood testing based on risk factors and age vary in frequency from every 6 months to every 3 years.
Height, weight, and BMI should be noted for risk factor assessment and for monitoring following diagnosis
Examination should rule out complications such as:
- Retinopathy by optometry/ophthalmology eye exam
- Peripheral arterial disease by palpation of pulses
- Neuropathy by sensation exam (eg. monofilament test)
- Diabetic foot
Risk factors
For screening purposes:
- Obesity and excess adipose tissue - most important risk factors, with association to abdominal fat distribution
- Family history - 2-3 fold increase in risk with first-degree relative with T2DM
- High risk populations - non-white, low SES
- History of gestational diabetes mellitus and/or prediabetes
- Cardiovascular risk factors
- Medications (and other conditions) associated with diabetes
Additionally:
- Diet - consumption of red meat, processed foods, sugar-sweetened beverages can increase risk of T2DM
- Physical activity - inactivity associated with increased risk, independent of weight gain
Diagnosis
Criteria
If asymptomatic, two results is needed for diagnosis (eg. two A1C after 3 months or A1C and FPG together immediately).
If symptoms of hyperglycemia present, then one result in diabetic range needed.
For A1C:
- Prediabetes: 6.0-6.4%
- Diabetes: ≥6.5%
For FPG (≥8 hr fasting): - Impaired fasting glucose: 6.1-6.9 mmol/L
- Diabetes: ≥7.0 mmol/L
OGTT: - Impaired fasting glucose: 7.8-11.0 mmol/L
- Diabetes: ≥11.1 mmol/L
A CBC is obtained to validate the A1C. A1C is a function of Hb turnover (longer RBC age is associated with falsely elevated A1C).
Work-up
Initial workup of blood glucose test can be done for screening and/or diagnosis.
For both the initial workup and further reassessment:
- Basic metabolic panel (incl. renal function and electrolytes)
- Urinalysis for glucosuria, ketones, microalbuminuria
- CBC with platelets
- Liver tests
- Lipid panel
If metformin is used, consider vitamin B12
C-peptide testing and islet autoantibody testing can distinguish between type 1 and type 2 if there is a clinical suspicion.
Differential
- Iatrogenic causes such as medications
- Genetic aberrations in beta-cell function and insulin action
- Infection
- Endocrinopathies such as acromegaly. Cushing disease, pheochromocytoma, hypothyroidism, etc.
- Conditions affecting the exocrine part of the pancreas such as pancreatitis, tumours, etc.
Red Flags / Complications
Uncontrolled or poorly controlled diabetes can manifest in a number of complications, both acute and chronic.
Acute complications include hyperglycemic crisis (incl. diabetic ketoacidosis and hyperosmolar hyperglycemic state) and hypoglycemia.
Chronic macrovascular complications are coronary artery disease, peripheral artery disease, and cerebrovascular disease.
Chronic microvascular complications are:
- Neuropathy (peripheral sensory loss which includes increased risk of foot ulcers and autonomic dysfunction which includes gastroparesis, cardiovascular, and sleep disturbances)
- Retinopathy (vision loss and blindness, cotton wool spots)
- Nephropathy
Management
Targets
In most adults, an A1C target of ≤7.0% is ideal to minimize risk of symptomatic hyperglycemia and complications.
For patients who are functionally dependent, frail, or have cognitive impairment, consider an A1C target of 7.1-8.5%.
For patients with potential for remission to prediabetes or normoglycemia, consider an A1C target ≤6.5 or 6.0% respectively. May also consider lower targets for further risk reduction (eg. risk of CKD) if patient is at a low risk for hypoglycemia.
Blood glucose targets for most patients:
- Fasting/preprandial: 4.0-7.0 mmol/L
- 2 hour postprandial: 5.0-10.0 mmol/L
Lifestyle / Social
Diet and physical activity modifications should be recommended for all diabetic patients regardless of pharmacological therapy. Management of weight can reduce insulin resistance and impaired beta cell function.
Diet
Patients should be educated on caloric restriction and in reducing consumption of sugar-sweetened beverages and other high glycemic index foods.
Exercise
Patients should be encouraged to decreased sedentary time and perform 30-60 minutes of moderate-intensity aerobic activity on most days, totalling at least 150 minutes per week. Consider resistance training especially in patients who are not overweight in the absence of contraindications.
Pharmacological / Interventional
Pharmacologic therapy should be initiated if A1C are at or above target levels in addition to lifestyle modifications. For highly motivated patients with A1C near target, a 3-6 month trial of lifestyle modifications can be considered prior to pharmacologic therapy.
Pharmacological therapy consist of antihyperglycemics and/or Insulin. Insulin is often a late-stage treatment (following beta-cell dysfunction) as T2DM is characterized by insulin resistance which insulin does not address.
Choice of medication often follows a sequential addition of agents:
- Initial monotherapy of metformin
- 500 mg daily with PM meal; can be increased up to 200mg per day as tolerated
- Addition of further antihyperglycemic agent(s)
- Selection may be due to comorbidities (such as kidney disease or heart failure) or risk factors (such as hypoglycemia risk)
- Add basal insulin
- Start with 10 units qHS
- Titrated to fasting glucose in target range (4-7 mmol/L) by increasing dose by 1 unit every night
- Add bolus insulin once daily
- Use bolus of 10% basal dose with largest meal of day
- Multiple bolus insulin at all meals
- Calculate total daily insulin (TDI) = 0.5 units/kg
- 40% TDI as basal insulin
- 60% TDI bolus split with each meal
Note that with sequential steps, previous step medications should be continued to be optimized. With addition of insulin, consider hypoglycemic risk and interactions with antihyperglycemic agents such as secretagogues.
References
Tools / Guidelines
Diabetes Canada: https://guidelines.diabetes.ca/GuideLines/media/Docs/Quick%20Reference%20Guide/2024-CPG-Quick-Reference-Guide.pdf
Insulin Prescribing: https://guidelines.diabetes.ca/GuideLines/media/Docs/Key%20Messages/Insulin_Prescription_EN_09_23.pdf