creation date: 2026-04-25 16:41
tags: Workups
Weakness
Background
Weakness refers to a lack or reduction of muscle strength.
Pathophysiology
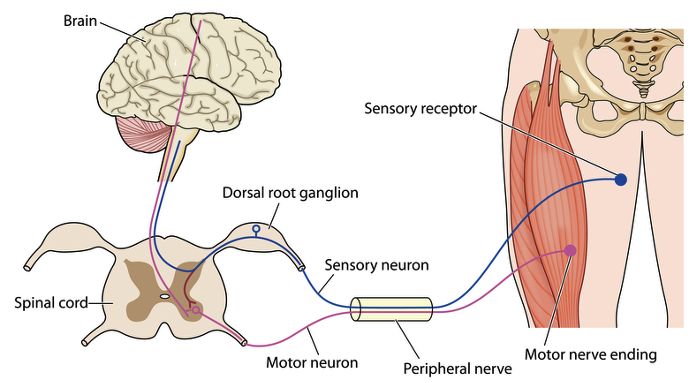
Muscle weakness can be due to a number of conditions or disease processes. Muscle contraction involves both neurologic and musculoskeletal systems. Problems may involve:
- Upper motor neurons (CNS) - motor nerves of brain and spinal cord
- Lower motor neurons (PNS) - anterior horn cell, nerve root, plexus, or peripheral nerve
- Muscle fibres/action
Differential Diagnosis
The diagnoses specific to certain investigations are discussed below.
Generalized weakness
- Toxic/medication induced
- Chronic illness
- Frailty/sarcopenia
- Endocrine disorders
- Electrolyte disturbances
Focal weakness
Common distributions:
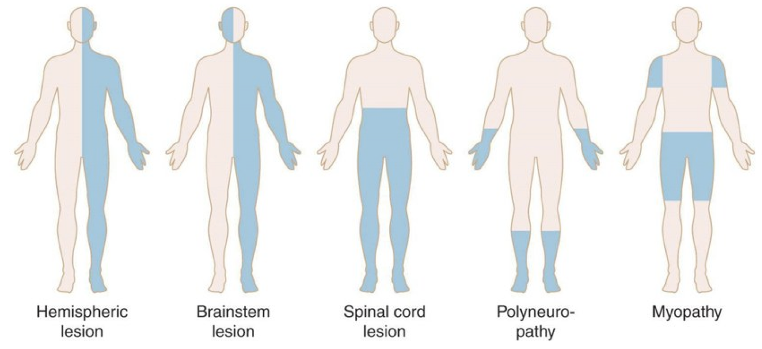
Bilateral:
- Spinal cord injury
- Neuromuscular junction (NMJ) disorder (proximal)
- Myopathy (proximal)
- Polyneuropathy (distal)
Unilateral:
- Stroke
- Acquired brain injury
- Traumatic brain injury
Focal limb:
- Radiculopathy
- Plexopathy
- Mononeuropathy (distal, more common entrapment sites)
- Tendon tear
Initial Evaluation
History
When the chief complaint is weakness, it is important to determine if the issue is true weakness. Confirm that the complaint is not:
- Fatigue
- Pain
- Arthritis/contracture
- Numbness
- Depression (mood)
- Cardiorespiratory
- Fibromyalgia/chronic fatigue syndrome
True weakness should be relatively constant (hour-to-hour basis). Note that the inability to exert due to pain is not weakness.
Characterization of the weakness
Onset
- Acute, subacute, chronic
- Relation to trauma, routine changes, illness
Pattern
- Generalized vs. focal
- Proximal vs. distal
- Bilateral vs. unilateral
- Limb, trunk, bulbar
Functional impairment
Ask about challenges to gauge pattern of weakness. Examples include tripping, falls, difficulties with stairs, overhead activities, opening jars, and/or using buttons/zippers.
Associated symptoms
May include:
- Pain
- Fatigue
- Numbness, tingling
- Loss of muscle bulk
- Incoordination
- Bulbar, respiratory symptoms
- Autonomic, bowel, bladder
- Systemic, constitutional symptoms
Physical Exam
Physical exam consist of:
- Power grading (/5)
- “Give-way weakness” - indicates pain, FND, anxiety/kinesiophobia
- Gait, sit-to-stand, squats
- Full neurological exam
Signs of UMN lesion includes:
- Less pronounced muscle atrophy
- Hyperreflexia
- Hoffman sign (flicking middle finger nail causes involuntary flexion and adduction of thumb and index finger)
- Babinski sign
- Clonus (involuntary, rhythmic muscle contraction; especially plantarflexors)
- Impaired coordination
- Spasticity (velocity dependent increase in muscle tone)
Signs of LMN lesion include:
- Atrophy
- Hyporeflexia
- Hypotonia
- Fasciculations
Investigations
Investigation depends on the suspected pathology.
Central nervous system
- MR brain: CVA, traumatic bleed, mass lesion, inflammation
- MR spine: spinal cord compression, spinal cord mass, inflammation, ischemia
Peripheral nervous system
- MR spine, MR plexus, MR neurography, nerve ultrasound
- Electromyography (EMG) and nerve conduction studies:
- Motor neuron disorders/ALS, radiculopathies, plexopathies, neuropathies, myopathies
Laboratory tests
Lab tests are often performed to rule out other causes:
- Electrolytes
- TSH, cortisol (endocrinopathies)
- A1C, fasting glucose, OGTT (diabetes)
- Vitamin B12
- Inflammatory markers
- CK (myopathies)
- Anti-AChR antibodies (myasthenia gravis; NMJ disorder)
- Infection (HIV, lyme)
- Genetic testing (hereditary neuropathy, myopathies)