creation date: 2026-05-04 22:32
tags: Workups
Facial Trauma
Background
The face is crucial for appearance and function. Injuries can affect eating, speaking, social interactions, and more.
For young adults, sports (football, baseball, hockey) account for a large proportion of causes. Other causes include MVAs, interpersonal/domestic violence, falls, animal bites, and other recreational activities.
Anatomy and Physiology
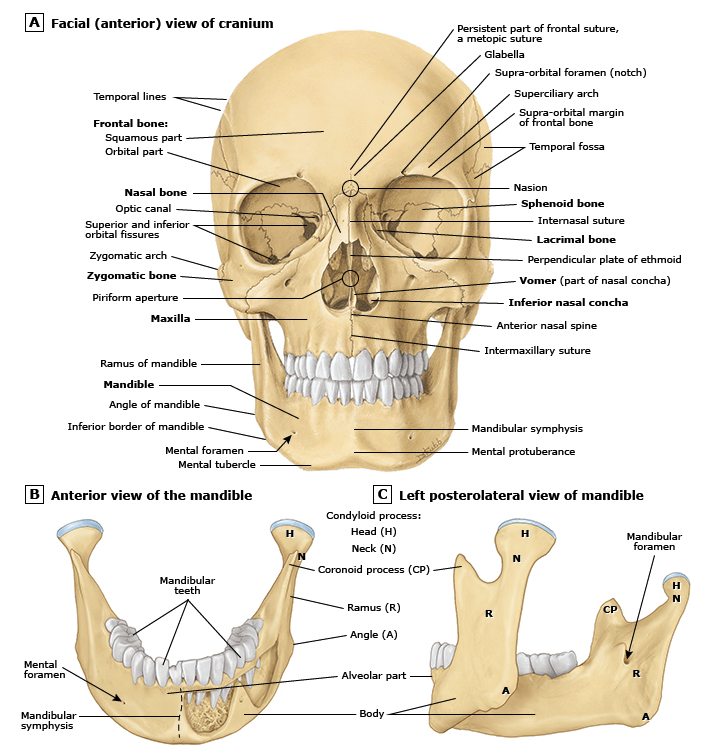
Bones
The posterior portions of the face form the anterior wall of the calvaria (skull bones).
The anterior facial skeleton consist of the frontal bone, nasal bone, zygomas, maxillary bones, and mandible. The deeper structures consist of the sphenoid, ethmoid, lacrimal, vomer, and temporal bones. These are relevant for muscular attachment.
The temporomandibular joint (TMJ) is the only joint that engaged in complex motion. The mandible rotates and translates anteriorly when the mouth opens.
Nerves
Innervation of the face is as follows:
| Nerve | Function |
|---|---|
| Cranial nerve V | Sensation to the face through V1 (ophthalmic), V2 (maxillary), V3 (mandibular). |
| Cranial nerve VII | Anterior muscle layer for facial expression; note, travels through narrow canal within temporal bone which is susceptible to injury |
| Cranial nerve V, IX, X | Innervates muscles for mastication; V = jaw movement, IX and X = palatal movement) |
Vasculature
The face is highly vascularized and is at risk of hematoma or heavy bleeding. It should be noted that because of extensive anastomoses (collateral blood supply), ischemia is unlikely to occur.
Muscles
Facial musculature is complex. The relevant muscles to trauma are:
- Extraocular muscles
- Peri-mouth muscles
Skin
Skin on the face is the thinnest in the body. Lacerations that run parallel to Langer’s line (which is along which natural aging creases form) tend to scar less prominently than those that do not.
Pathophysiology of Injury
Injury may be due to blunt force or penetrating injury, or some combination of the two.
Fractures may complicate airway management (although mandible fractures may allow for easier access). Bleeding can also complicate intubation.
Initial Evaluation
Immediate trauma assessment should occur as with any trauma. Below describes additional components specific to facial trauma.
History
Additional questions include:
- Can you breathe through both sides of your nose? (nasal fracture)
- Are you having any trouble speaking? (mandibular fracture)
- Do you have double vision or any other trouble with your vision? (orbital or nasoorbitoethmoid fracture)
- Is your hearing normal?
- Are you experiencing any numbness of your face? (nerve injury)
- Have you had any previous facial injuries or surgeries, including ocular procedures? (risk of ocular injury and globe rupture)
- Do your teeth come together the way they did yesterday? (malocclusion; mandibular fracture)
- Are any of your teeth painful or loose?
- Were you bleeding from your mouth, nose, or ears?
- Have you experienced any vertigo? (raise suspicion of temporal bone fracture)
Physical Exam
Inspection
General:
- Asymmetry or gross discrepancies in motor function
- Lacerations, abrasions, contusions, tissue avulsions
- Relative positions of eyeballs
- Intercanthal distance
Eyes:
- Visual acuity
- Extraocular movements
- Close inspection for open globe, afferent pupillary defect, hyphema, corneal abrasion, orbital step off
Nose:
- Septal hematoma (requires urgent drainage)
- Rhinorrhea (CSF leak possible)
Mouth, maxilla, mandible:
- Dysphonia or edema
- External lacerations to parotid area
Ears:
- Lacerations and hematomas
- Battle sign (postauricular ecchymosis - basilar skull fracture)
- Otoscope for CSF leak
Palpation of bony prominences
- Focal tenderness
- Step-off
- Crepitus
- Abnormal motion
Nerve assessments
- CN VII (facial motor)
- CN V (sensation)
Investigations
Facial traumas are assessed using CT scans. Ocular/orbital injury may benefit from bedside ultrasound, particularly if the patient is not able get a CT scan done.
In cases of isolated nasal injury, nasal bone x-rays are not required if all the following criteria are met:
- Tenderness and swelling is isolated to the bony bridge of the nose
- The patient can breathe through each naris
- The nose is straight (no septum deviation)
- No septal hematoma