creation date: 2026-02-06 20:20
status: note
tags: ACP Mental, Neurological & Musculoskeletal Health, Directed Independent Learning
Pediatrics MSK
Module - Common Pediatric MSK Concerns
Objectives
- Describe the normal development of gait in childhood
- Diagnose commonly encountered childhood limps and identify those that require urgent management
- Distinguish patients with lower limb abnormalities that require investigation and treatment
- Differentiate common infant foot deformities and explain their significance
- Recognize different types of spinal deformity
- Categorize the risk of curve progression in adolescent idiopathic scoliosis
Normal
Gross Motor Development
Is a part of developmental milestones.
- Walk independently by 18 months
Gait
Gait is a cyclical movement of the right and left feet to move the body forward. In normal gait, the cycle is symmetrical.
Stance phase: period during which a limb bears weight
- Single limb stance: when the contralateral limb is off the ground
Double support: when both feet are touching the ground simultaneously - Children tend to spend more time in double support
- The proportion of time spent in single limb support increases with age (35% in 3 year olds, to 39% in adults)
Swing phase: when the limb swings forward for the next step (coincides with single stance of the other leg)
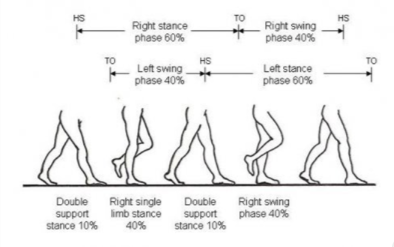
Heel strike: the moment when the heel of the swing leg strikes the floor first
Toe off: the pushing off of the toe about to make the step following the heel strike and rolling of foot
Base of support: refers to the distance in the medial-lateral direction between the right and left foot in double support
Stride length: distance from the point of one heel strike to the next spot where the same heel strikes
Step length: distance from point of one heel strike to the point of the heel strike of the opposite foot
Development
At 12 months:
- Holds arm straight out in front
- Hips and knees flexed throughout gait cycle
- Foot strikes with plantarflexed ankle (no heel strike)
At 18 months: - Heel strike is evident
- Reciprocal arm swing (in most children)
Pathology
Abnormal Gait
Antalgic gait: asymmetric gait in the timing with less time spent on affected side
- Associated with unilateral pain somewhere in the lower extremity
Trendelenberg’s gait: shoulder and upper body shift laterally towards the affected side during that leg’s stance phase; results in a lateral swaying motion - Associated with weak hip abductors (incapable of stabilizing pelvis levels during single leg stance); contralateral side drops during swing phase
- Hip pathology
Steppage gait: hip and knee flexes excessively during swing phase (looks like stepping up stairs) and entire foot contacts the ground at once (no heel strike, known as foot-drop) - Can be associated with deep peroneal nerve damage
- Can be associated with underlying neurological disorder (eg. cerebral palsy, hereditary motor sensory neuropathy)
Refusal to Ambulate
Toddlers may refuse to ambulate if ambulation causes pain. This is a severe form of antalgic gait.
- Crawling but not walking suggests injury to tibia or foot but normal femur and hip
Differential Diagnosis
Most important diagnoses:
- Developmental hip dysplasia
- Septic hip
- Toxic synovitis
- Slipped capital femoral epiphysis
- Legg-Calve-Perthes disease
Other diagnoses:
- Juvenile inflammatory arthritis
- Primary bone tumour
- Leukemia
- Lymphoma
- Cerebral palsy
- Rickets
- Fracture or soft tissue injury
- Rotational malalignment
Approach to limping child
Relevant questions to answer to diagnose:
Pain
Is the limp due to pain? If so:
- Is the pain constant, intermittent, transient?
- What time during the day or following what activity is it worst?
- Has the quality/intensity changed over time?
Pain that is constant, non-mechanical, and/or wakes the patient from sleep is worrisome (bone infections, neoplasms).
Some limps are painless (eg. Legg-Calve-perthes disease).
Onset
Did the limp develop suddenly, gradually, or has always been there?
Sudden or acute onsets:
- Trauma
- Acute infection
Chronic and gradually worsening:
- Inflammatory
- Mechanical
- Neurologic
- Neoplastic
Systemic illness
Is there systemic signs such as:
- Fever
- General malaise
- Weight loss
It is important to appraise medication use as they may mask symptoms (eg. antibiotics may mask infectious processes).
Type
What type of limp does the child have? Different presentations may point towards different pathologies.
Location
Can a site of origin be located through physical exam:
- Point of maximum tenderness
- Sources of referred pain
- Is the pain aggravated by specific motion of specific joint
Conditions
Legg-Perthes disease
- Avascular necrosis of the femoral head
- Affects younger children (aged 4-8), more commonly in boys
- Unilateral, painless limp
- XR: normal initially, femoral head collapse in following weeks to months
- Prognosis is favourable for younger patients but worse >8 years; outcome depends on shape of femoral head at healing
- Treatment involves maintaining a congruent hip joint via physiotherapy or surgical reconstruction
Slipped capital femoral epiphysis
- Acute or chronic presentation of:
- Pain felt through groin that is worse with activity
- Trendelenburg gait with external rotation of affected limb
- Affects children as they enter adolescence; typically associated with overweight but not always
Developmental dysplasia of the hip
- Manifests as a spectrum from frank dislocation of one or both hip to subluxation
- Typically diagnosed in infancy; genetic tendency
- Barlow and Ortolani maneuvers
- Ultrasound can also visualize acetabular development and femoral head position - used for diagnosis and screening of high risk babies
- In older children, manifests as painless Trendelenburg gait
Septic hip
- Acute illness
- Fever
- Laboratory evidence of infection (elevated WBC, increased neutrophil on differential, elevated ESR and CRP)
- Rapid onset
- Characterized by antalgic gait or refusal to ambulate
- Physical exam finds extreme pain and guarding upon passive motion
- Radiographically normal; ultrasound finds fluid in hip joint
- Diagnosis: hip aspiration and fluid cell count and culture confirms
- Most commonly infected with Staph aureus
Toxic synovitis
- AKA transiet synovitis
- Presents similarly to septic hip but without systemic symptoms and bloodwork abnormalities
- May be preceded by viral illness (often upper respiratory)
- Hip aspiration is required to r/o septic arthritis but presumed to be post-viral syndrome if fluid cultures are negative
- Treated with rest and observation
Intoeing
Intoeing is not thought of as a limp but moreso a gait variation.
- Adults walk with toes pointed forward and slightly externally rotated
- Children can intoe (not abnormal)
Common causes of intoeing are:
- Foot deformity known as forefoot adductus resulting in foot to curve medially; resolved with stretches
- Internal tibial torsion due to prenatal positioning; typically self-resolves by age 5
- Femoral anteversion (>10 degree seen in adults) which is normal anatomically for children; corrects over time
Infant foot deformities
Foot deformities are typically noted at birth and can be bilateral or unilateral. Common deformities include:
Forefoot adductus
- Curving of foot
- Resolves with simple stretching exercises
- Persistent cases requires casting by 4-6 months
Calcaneovalgus foot
- Most common infant foot deformity
- Foot held dorsiflexion, often with the dorsum of the foot touching the anterior shin; heel is in valgus
- Flexible
- Resolves quickly with time and stretching
Vertical talus
- Similar in appearance to calcaneovalgus foot but rigid
- Talonavicular joint is dorsally dislocated and talar head is palpable as a firm prominence in the inset of the foot
- Requires casting and surgical correction; genetic consultation required due to associated genetic conditions
Clubfoot
- Complex deformity involving the forefoot and hindfoot
- Typically an isolated abnormality but can be associated with genetic diagnosis
- Serial casting is effective for treatment but surgery may be necessary after 6 months of age
Angular deformity
- Genu varum and valgum can be physiologic at certain ages
- Genu varum up until age 2
- Genu valgum may develop around age 2-3 and peaks around 3 years.
- Children with other abnormalities (eg. short stature) should have investigations for generalized skeletal abnormality workup but otherwise radiographs are not routine
Spinal deformity
Spine is normally straight when observed from behind. Asymmetry may be noted in the shoulders, scapulae, or waist.
Note: postural round back mimics kyphosis and is common in adolescents who “slouch”.
Kyphosis
-
40 degrees of dorsal convexity of the spin when viewed in the sagittal plane
- Differentiated from postural round back by noting sharp saggital plane curve on forward flexion that is not correctable by shoulder hyperextension
- X-rays are diagnostic: anterior height of several adjacent vertebrae at least 5 degree of wedging and uneven endplates
Scoliosis
- Lateral/medial curve of the spine
- Physical exam - observe spine when:
- Both feets are flat
- Knees held symmetrically in extension
- Asymmetry may be noted at the level of the shoulder, scapula, waist, and/or pelvis, especially if patient bends forward while keeping knees extended
- Neurologic exam should be performed as well
- Xray can quantify curve - Cobb angle measures the maximum vertebrae tilt
- 10 degree - unlikely to have problems
- 20 degree or more - may have long term complications if still have much growth remaining
- 40 degree or more - may cause problems in mid-life
- Braces can be used to halt curve progression; surgical correction and fusion of spine may be indicated if braces are insufficient