creation date: 2026-04-25 21:45
tags: Assessments
Oral Lesions
Background
Evaluation of a Suspicious Lesion
History
HPI
- Onset, location, intensity, frequency, duration
- Aggravating and/or relieving factors
- Change over time
Medical, tobacco, and alcohol history
- Medical conditions
- Medications and allergies
- Tobacco and alcohol use (major risk factors for malignancy)
Physical Exam
Extraoral examination
- Inspection of head and neck region for asymmetry or swelling
- Palpate the submental, submandibular, cervical, and supraclavicular regions for lymph nodes
- Inspect and palpate the lips and perioral tissues
Intraoral examination
- Inspect and palpate all oral soft tissues
- Pay particular attention to high risk sites (lateral and ventral aspects of the tongue, floor of mouth, soft palate)
Characterization of lesion
If a lesion is identified, characterize it by:
- Size: length and width
- Colour: white (eg. leukoplakia if not classified as any other lesion), speckled, red (erythroplakia if not any other lesion); homogenous vs. nonhomogenous
- Outline (borders): discrete vs. diffuse
- Texture: smooth, flat, raised, dome-shaped; granular, verrucous, ulcerated, indurated
Priority for biopsy/referral should be given for:
- Speckled red and white appearance
- Nonhealing ulceration
- Induration
Examples of clinical features, in order of increasing risk are:
- Smooth, white, discrete, homogenous lesion
- Predominantly red, diffuse, granular lesion
- Diffuse, red ulcerated lesion
- Diffuse, raised, speckled, indurated lesion
Additional Investigations
Visual tools
Toluidine blue stain retention
- Stains nucleophilic tissue components (eg. DNA)
- Valid for detection of oral cancers; unclear value for premalignancy but generally shows retention by any premalignant lesion
Direct fluorescence visualization - Detects alteration to tissue structure and biochemistry associated with premalignant disease
- All high-grade oral premalignant lesion and cancer detected
Diagnostic biopsy
Indication for diagnostic biopsy are:
- Suspicious lesion from history and physical
- Persistence for >3 weeks following removal of local irritant
Differential Diagnosis
Oral mucosal lesions can be grouped into 5 categories (known as the 5 I’s):
- Inherent (congenital or hereditary)
- White sponge nevus
- Inflammation
- Oral lichen planus
- Some variants of geographic tongue
- Infection
- Oral candidiasis
- Iatrogenic
- Drug-induced lichenoid reaction
- Friction hyperkeratosis
- Idiopathic
- Oral premalignant lesion
- Neoplasm
The first 4 categories must be ruled out before a lesion is classified as leukoplakia or erythroplakia.
Common Lesions
Aphthous Stomatitis (Canker Sores)

Clinical Findings
- Round to oval ulcers with a grey-white fibrinous pseudomembranous base and a well-defined erythematous halo
- Affect non-keratinized moveable mucosa (buccal mucosa, ventral tongue, floor of mouth, soft palate, labial mucosa)
- Three subtypes: minor (<10 mm, most common), major (>10 mm, deeper, scarring), herpetiform (multiple tiny clustered ulcers)
- Intensely painful, disproportionate to size; worsened by acidic and spicy foods
- Self-limiting (minor: 7–14 days); recurrent episodes typically monthly or more frequently; no systemic involvement in minor aphthae
Pathophysiology
- Exact cause is not fully understood, but RAS involves dysregulated T-cell-mediated cytotoxicity directed against oral mucosal epithelium
- CD4+ and CD8+ T lymphocytes, along with TNF-α and IL-2, drive local tissue destruction
- Triggers include minor trauma, stress, hormonal changes, nutritional deficiencies (B12, folate, iron), and food sensitivities
- The ulcer results from full-thickness epithelial loss with an acute inflammatory infiltrate at the base; unlike HSV, there is no viral cytopathic effect and the ulcers are confined to non-keratinized mucosa
Diagnosis/Treatment
- Clinical diagnosis based on characteristic morphology and recurrent history
- Rule out nutritional deficiencies (CBC, B12, folate, iron) and systemic associations (IBD, Behcet disease, celiac)
- Topical high-potency corticosteroids (triamcinolone in Orabase) or lidocaine for symptomatic relief
- Colchicine or dapsone for severe/refractory cases
Differential Diagnosis
- Herpes simplex virus (HSV) oral ulcers
- Behcet disease
- Erosive lichen planus
Herpes Labialis (HSV-1 Reactivation)

Clinical Findings
- Prodrome of tingling, burning, or pruritus at the lip 12–24 hours before visible lesions
- Clustered small vesicles on an erythematous base at or near the vermilion border, typically on the lower lip
- Vesicles rapidly rupture forming painful, crusted erosions that heal over 7–10 days
- Recurs predictably at the same location; triggered by UV exposure, febrile illness, stress, or immunosuppression
- Intraoral involvement is uncommon in recurrent episodes (unlike primary herpetic gingivostomatitis, which causes widespread oral ulceration and systemic symptoms)
Pathophysiology
- Following primary infection (often subclinical in childhood), HSV-1 establishes latency in the trigeminal ganglion sensory neurons
- Reactivation occurs when cellular stressors trigger viral replication within the neuron
Diagnosis/Treatment
- Clinical diagnosis
- Tzanck smear (multinucleated giant cells) or HSV PCR/culture if uncertain
- Start oral valacyclovir or acyclovir if present within prodrome to shorten duration and severity
Differential Diagnosis
- Impetigo
- Recurrent aphthous stomatitis (aphthae are on non-keratinized mucosa, no prodrome)
- Erythema multiforme (post-herpetic)
Leukoplakia

Clinical Findings
- White patch or plaque that cannot be wiped off and cannot be attributed to any other definable lesion (diagnosis of exclusion)
- Homogeneous type: uniformly flat, thin, white with a smooth or finely wrinkled surface; lower malignant potential
- Non-homogeneous types: speckled (erythroleukoplakia), nodular, or verrucous; higher malignant potential
- Most common sites: buccal mucosa, floor of mouth, ventral tongue, lower lip; floor of mouth and ventral tongue carry the highest transformation risk
- Usually asymptomatic; associated with tobacco use (smoking or smokeless), alcohol, and chronic friction
Pathophysiology
- The white appearance results from epithelial thickening (acanthosis) and increased surface keratin production (hyperkeratosis or parakeratosis), which prevents light from penetrating through to the underlying vasculature
- Thickening due to repeated mucosal irritation which can eventually cause DNA damage and lead to invasive SCC
- Approximately 1–3% of leukoplakia lesions transform to malignancy per year
Diagnosis/Treatment
- Incisional or excisional biopsy is mandatory to assess for dysplasia or SCC
- Eliminate causative factors (tobacco cessation)
- Dysplastic or high-risk lesions (floor of mouth, ventral tongue, non-homogeneous pattern) require surgical excision or laser ablation with close follow-up every 3–6 months
Differential Diagnosis
- Oral candidiasis (pseudomembranous; white coating is wipeable)
- Lichen planus (reticular/lacy pattern, bilateral, symptomatic)
- White sponge nevus (rare, hereditary, bilateral, benign)
Erythroplakia

Clinical Findings
- Bright red, velvety, well-demarcated patch on the oral mucosa that cannot be attributed to any other cause
- Smooth or slightly granular surface; may have areas of ulceration in advanced cases
- Most commonly on the floor of the mouth, ventral/lateral tongue, and soft palate
- Usually painless or only mildly sensitive; lack of pain often delays presentation
- Highest risk oral mucosal lesion: >80% harbour severe dysplasia, carcinoma in situ, or invasive SCC at time of biopsy
Pathophysiology
- Erythroplakia appears red rather than white because the epithelium is atrophic (keratin layer is thinned or absent) allowing the underlying vascular lamina propria to show through
- Atrophy is a manifestation of advanced epithelial dysplasia or in situ/invasive carcinoma in the majority of cases
Diagnosis/Treatment
- Urgent biopsy is mandatory given the very high rate of severe dysplasia or carcinoma in situ at presentation
- If SCC confirmed, urgent referral to oral/maxillofacial surgery or head and neck oncology for staging and resection
- Adjuvant radiotherapy or chemotherapy depending on stage
- Complete tobacco and alcohol cessation
Differential Diagnosis
- Atrophic/erosive lichen planus
- Denture-related erythematous candidiasis
- Early oral squamous cell carcinoma
Oral Lichen Planus (Erosive/Reticular)

Clinical Findings
- Six classical forms: reticular (most common), erosive, atrophic, bullous, plaque-like, and papular
- Reticular form: interlacing white lines (Wickham striae) on the buccal mucosa — bilateral and symmetric (pathognomonic)
- Erosive form: painful, persistent erythematous erosions or shallow ulcers with a fibrinous base, often surrounded by white striations
- Chronic course with exacerbations; worsened by spicy and acidic foods
- Associated with hepatitis C virus, certain medications, and dental restorations; ~1-2% risk of malignant transformation (especially erosive form)
Pathophysiology
- T-cell-mediated chronic inflammatory condition in which autoreactive CD8+ cytotoxic T lymphocytes attack basal keratinocytes of the oral epithelium
- Antigen presentation triggered by medications, dental materials, viral antigens such as HCV, or unknown autoantigens
- Cells release perforin and granzyme B, directly inducing keratinocyte apoptosis
- Reticular (Wickham striae) form is caused by irregular thickening of the epithelium overlying the areas of inflammation; erosive lesions occur where the epithelium has broken down
- OLP has ~1–2% malignant transformation risk, particularly the erosive form
Diagnosis/Treatment
- Clinical diagnosis in classic cases, but biopsy (H&E ± DIF) is recommended to confirm and exclude dysplasia
- Eliminate potential triggers (review medications and dental restorations)
- ?Observation and monitoring
- First-line: topical high-potency corticosteroids (clobetasol or fluocinonide)
- Topical calcineurin inhibitors (tacrolimus) for steroid-refractory cases
- Long-term follow-up every 6–12 months for malignant transformation surveillance
Differential Diagnosis
- Leukoplakia
- Candidiasis (pseudomembranous)
- Lupus erythematosus (oral lesions)
Oral Squamous Cell Carcinoma (OSCC)
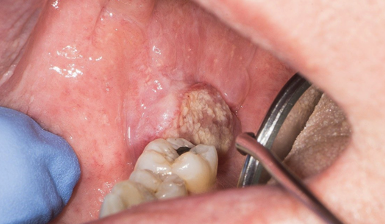
Clinical Findings
- Non-healing ulcer with indurated, raised, and irregular edges - induration (hardness) on palpation is a critical clinical sign
- Most common sites: lateral border and ventral tongue, floor of mouth, lower lip vermilion, and soft palate
- May begin as leukoplakia, erythroplakia, or a mixed (speckled) lesion before ulcerating
- Later features: pain, dysphagia, odynophagia, ipsilateral otalgia (referred pain via CN V), trismus, cervical lymphadenopathy
- Strong risk factors: tobacco (smoking/smokeless), alcohol (synergistic), and HPV-16 infection (especially oropharyngeal SCC)
Pathophysiology
- Malignant transformation of squamous mucosal epithelium through the progressive accumulation of genetic and epigenetic alterations by:
- Carcinogen-driven, where tobacco and alcohol cause direct DNA damage, TP53 mutations, and chromosomal instability, particularly in older adults
- HPV-driven (predominantly HPV-16), where viral oncoproteins E6 and E7 inactivate p53 and pRb respectively, leading to uncontrolled cell-cycle progression
- Lateral tongue and floor of mouth are highest-risk sites due to pooling of carcinogens in saliva and thin mucosa
Diagnosis/Treatment
- Urgent incisional biopsy for histopathological confirmation
- Imaging (CT/MRI of head/neck) for staging and lymph node assessment
- Urgent referral to head and neck surgery/oncology
- Treatment is wide local excision with adequate margins ± neck dissection for node-positive disease, followed by adjuvant radiotherapy ± chemotherapy (cisplatin) based on pathologic stage
Differential Diagnosis
- Traumatic ulcer (should heal within 2 weeks)
- Major aphthous ulcer (Sutton disease)
- Salivary gland malignancy
Oral Candidiasis (Pseudomembranous Type / Thrush)

Clinical Findings
- Creamy white, curd-like pseudomembranous plaques on any oral mucosal surface (tongue, palate, buccal mucosa, oropharynx)
- Plaques can be wiped off with gauze, revealing an erythematous, raw, and sometimes bleeding base (key distinguishing feature from leukoplakia)
- Burning sensation, soreness, and altered or metallic taste (“cottony” sensation)
- Predisposing factors: recent antibiotic or corticosteroid use, immunosuppression (HIV/AIDS, chemotherapy, transplant), xerostomia, denture wearing, infancy, extremes of age
- In HIV/AIDS, extensive oral candidiasis is an AIDS-defining illness and a marker of significant immunosuppression
Pathophysiology
- Candida albicans is normally present in oral cavity but controlled by intact mucosal barriers, saliva, competing bacterial flora, and host immune responses
- Disruption of any of these defenses enables pathogenic conversion from yeast form to invasive hyphae/pseudohyphae
- Antibiotic use eliminates competing oral bacteria
- Immunosuppression, xerostomia, dentures, and inhaled corticosteroid use are other key risk factors
- White pseudomembrane is composed of desquamated epithelial cells, fungal hyphae, fibrin, leukocytes, and debris
Diagnosis/Treatment
- Clinical diagnosis confirmed by scraping off the pseudomembrane
- KOH preparation of the scraping reveals budding yeast with pseudohyphae
- Rule out immunosuppression if no obvious precipitant (consider HIV testing)
- Treat with oral nystatin suspension (swish and swallow) for mild/localized disease; oral fluconazole for moderate/severe or refractory cases
- Review antibiotic use, inhaled steroid technique, and denture hygiene
Differential Diagnosis
- Oral hairy leukoplakia (EBV-driven, lateral tongue, non-wipeable, in HIV patients)
- Chemical burn or milk coating in infants
- Lichen planus (white lesions, non-wipeable, bilateral, lacy)
Geographic Tongue (Benign Migratory Glossitis)

Clinical Findings
- Irregular, well-demarcated erythematous patches on the dorsal and lateral tongue, representing areas of filiform papillae loss (atrophy)
- Each patch is surrounded by a raised, white-yellowish serpiginous border of regenerating epithelium
- Lesions classically migrate, changing in shape, size, and location over days to weeks
- Usually asymptomatic; mild burning or sensitivity may occur with hot, spicy, or acidic foods
- Benign and chronic with no malignant potential
- May be associated with fissured tongue, psoriasis, and atopy
Pathophysiology
- Cyclic, localized loss and regeneration of filiform papillae on the dorsal tongue
- Atrophic red patches represent areas where filiform papillae have shed prematurely due to focal epithelial disruption, exposing the underlying atrophic mucosa
- Histology shows a psoriasiform pattern (likely similar inflammatory pathway to psoriasis, atopy, and fissured tongue
- Regenerating epithelium at the advancing margins forms the white border
- Cyclic migratory nature remains incompletely explained but stress, hormonal changes, and nutritional factors are implicated
Diagnosis/Treatment
- Clinical diagnosis based on the characteristic migrating map-like pattern; biopsy is rarely needed
- Reassure the patient that this is a benign, self-limited condition with no malignant potential
- Symptomatic relief with avoidance of triggering foods and use of topical anesthetics or antihistamine rinses if burning is significant
Differential Diagnosis
- Atrophic/erosive candidiasis (erythematous form)
- Erosive lichen planus
- Vitamin B12 or iron deficiency glossitis (diffuse atrophic glossitis without a migratory pattern)
Black Hairy Tongue

Clinical Findings
- Elongated, hypertrophied filiform papillae on the dorsal tongue, giving a “hairy” texture; can reach up to 2–3 cm in length
- Discolouration ranges from yellow-brown to dark brown or black, depending on the colonizing organisms and dietary pigments
- Coating is not easily wiped off (unlike candidal pseudomembrane)
- Associated symptoms: halitosis, metallic or altered taste, occasional nausea due to gag reflex stimulation from elongated papillae, mild xerostomia
- Ventral tongue and lateral borders appear entirely normal; no pain or ulceration
Pathophysiology
- Results from hypertrophy and elongation of the filiform papillae on the dorsal tongue combined with failure of normal desquamation
- Normally, filiform papillae are shed regularly through friction from food and the tongue’s movement
- When mechanical debridement is reduced (liquid diet, soft foods, dry mouth) or the oral flora is disturbed (antibiotics, proton pump inhibitors), papillae can grow to 1–3 cm instead of their normal 1 mm
- Chromogenic bacteria and yeasts (including Candida and tobacco pigments) colonize the elongated papillae and produce the dark pigmentation
- Predisposing factors include antibiotic use, heavy tobacco smoking, excessive coffee or tea intake, hydrogen peroxide–containing mouthwashes, and xerostomia
Diagnosis/Treatment
- Clinical diagnosis
- Identify and eliminate contributing factors (review medications, mouthwash use, tobacco, caffeine)
- Improve oral hygiene with gentle tongue brushing and increased water intake
- Condition is benign and reversible with cessation of precipitating factors
- Antifungal therapy only if concurrent candidal superinfection is confirmed
Differential Diagnosis
- Pseudomembranous candidiasis (white, wipeable)
- Pigmentation from bismuth, iron, or other medications
- Melanotic macule or oral melanoacanthoma
Mucocele (Mucous Extravasation Cyst)

Clinical Findings
- Painless, smooth, dome-shaped fluctuant swelling with a bluish or translucent hue
- Most common on the inner surface of the lower lip (minor salivary gland distribution); less commonly on the floor of the mouth (ranula), buccal mucosa, or ventral tongue
- Size typically 0.5–1.5 cm; soft and compressible on palpation
- Often fluctuates in size — may partially rupture, temporarily deflate, and refill
- Frequently preceded by local trauma (lip biting)
- Found most often in children and young adults
Pathophysiology
- Trauma to the lip severs a minor salivary gland duct, causing mucin to spill into surrounding connective tissue
- Mucin is a foreign substance in the stroma so it triggers a macrophage-dominated chronic inflammatory reaction that walls off the mucin pool with granulation tissue (not true epithelial lining and thus “pseudocyst”)
Diagnosis/Treatment
- Clinical diagnosis
- Simple observation if very small; most do not resolve spontaneously
- Definitive treatment is surgical excision of the cyst and the associated minor salivary gland tissue to prevent recurrence (common if gland not fully removed)
- Marsupialization or laser ablation are alternative treatment
Differential Diagnosis
- Ranula (larger, floor of mouth, involves sublingual gland)
- Salivary gland neoplasm (firm, not fluctuant)
- Lipoma (soft but not translucent, no mucin on aspiration)
Torus Palatinus and Torus Mandibularis
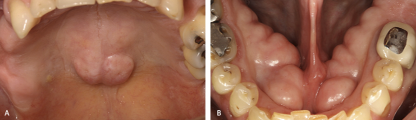
Clinical Findings
- Torus palatinus: exophytic bony hard nodule or lobulated mass on the midline of the hard palate
- Torus mandibularis: bilateral symmetric bony protuberances on the lingual aspect of the mandible, typically in the premolar region
- Non-tender, smooth, well-defined, and firmly attached to underlying bone; covered by thin, normal-appearing mucosa
- Completely asymptomatic — slow-growing over years; size remains stable once mature
- Prevalence: torus palatinus ~20% of the population (more common in women, East Asians); torus mandibularis ~8% (often bilateral and symmetric)
Pathophysiology
- Tori are benign, slow-growing bony exostoses (reactive hyperostosis)
- Arise from a combination of genetic predisposition (autosomal dominant with variable expressivity) and local mechanical stress (eg. bruxism (teeth grinding) and clenching)
- In response to these forces, periosteal osteoblasts are activated, producing localized nodular cortical bone overgrowth
- Tori consist of compact and cancellous bone without a medullary cavity.
- Overlying mucosa is susceptible to traumatic ulceration from hard foods or dental appliances
Diagnosis/Treatment
- Clinical and radiographic diagnosis
- Reassure the patient that tori are benign normal variants requiring no treatment in most cases
- Surgical reduction (tori reduction) is indicated only if the lesion interferes with denture construction, speech, mastication, or causes repeated traumatic ulceration
Differential Diagnosis
- Osteoma (solitary, may be associated with Gardner syndrome)
- Peripheral ossifying fibroma
- Palatal abscess (painful, fluctuant, associated with a non-vital tooth)