creation date: 2026-02-09 18:51
status: note
tags: ACP Mental, Neurological & Musculoskeletal Health, Directed Independent Learning
Neuroradiology
Module - Neuroradiology
Objectives
- Review basic neuroanatomy
- Review cerebral vascular anatomy
- Identify and differentiate between common intracranial pathologies including hemorrhages and tumours
Introduction to Neuroimaging
Imaging Modalities
The primary modalities are CT and MRI.
CT is commonly used as the initial screening study for neurological pathologies and can be done with or without intravenous contrast.
- Pros: easily accessible, inexpensive, and fast
- Cons: imperfect sensitivity/specificity for some pathologies, requires radiation
Non-contrast:
- Bones are white
- CSF is black
- Grey matter is lighter than white matter
Contrast: - Choroid plexus enhances
- Vessels are bright
MRI is often used for further evaluation following CT and similarly can be with or without contrast.
- Pros: sensitivity and specific, doesn’t require radiation
- Cons: expensive and time consuming, metal-related contraindications
T1: (fat is bright)
- Bones are black
- CSF is black
- Grey matter is darker than white matter (myelinated)
T2: (fat and water is bright) - Bones are black
- CSF is white
- Grey matter is brighter than white matter
FLAIR (fluid attenuation inversion recovery): - Similar to T2 but fluid is dark
- Sequence used for fluid suppression and can identify pathologies where lesions are covered by CSF
POST-GAD: - Gadolinium increases T1 signal (brighter where gadolinium accumulates)
Angiography
Conventional cathether angiogram
- Catheter inserted in femoral artery and positioned in the carotid to inject contras
- X-rays are taken to image the blood vessels
CT angiogram/venogram
- Contrast is administered before CT
- Timing of contrast injection will determine if contrast will be in the arteries of veins
MRI angiogram
- Similar to CT angiogram but with MRI; gadolinium-based contrast is used
- Time of flight angiography can be used to visualize the flow within the vessel without the use of contrast
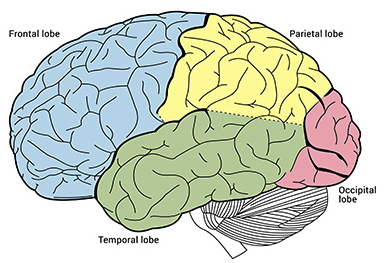
Basic Brain Anatomy
PACSBin - MR Brain
Radiopaedia - annotated MR brain
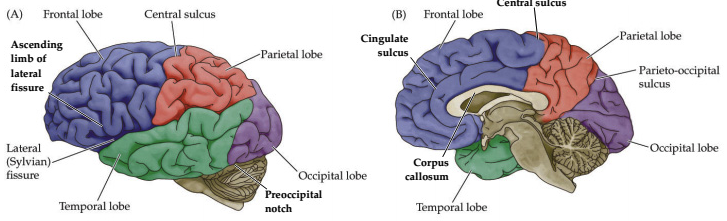
Lobes (frontal, parietal, temporal, occipital)
Cerebellum
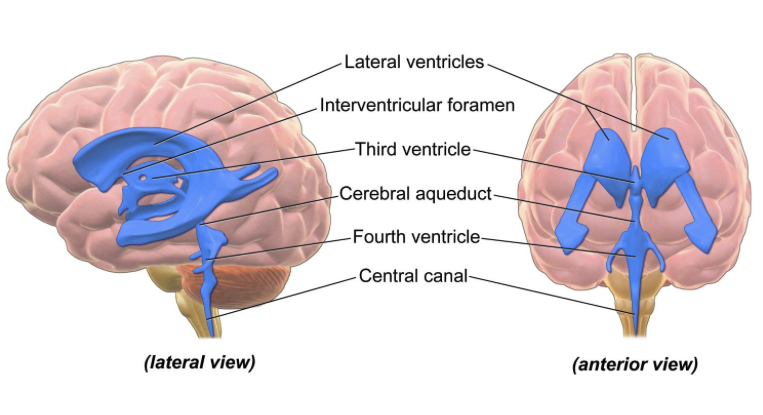
Ventricles (lateral, third, fourth)
Fissues (central, parieto-occipital, sylvian)
White matter tracts (corpus callosum, internal capsule)
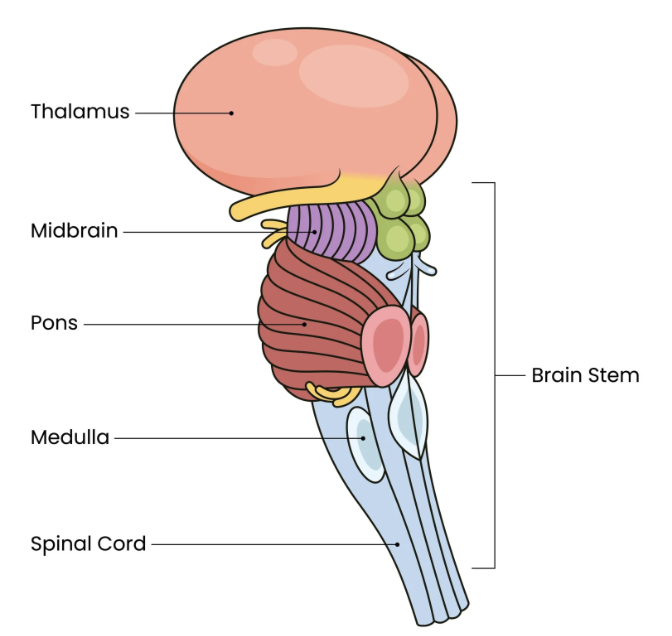
Basal ganglia (thalamus, caudate, lentiform nucleus)
Brain stem (medulla, pons, midbrain)
Dural folds (cerebral falx, cerebrellar tentorium)
Vascular Anatomy
Arterial Vasculature
Circulation begins at the aortic arch and connects as follows:
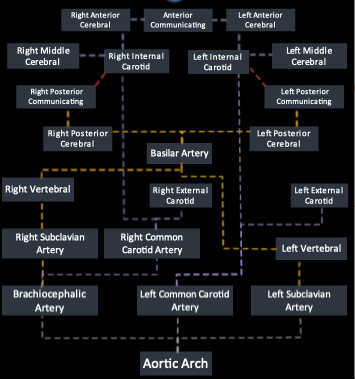
The Circle of Willis consist of the loop involving the:
- Posterior cerebral arteries
- Posterior communicating arteries
- Internal carotid arteries
- Anterior cerebral arteries
- Anterior communicating artery
This loop acts as redundancy and collateral circulation should one artery become occluded.
From an inferior view:

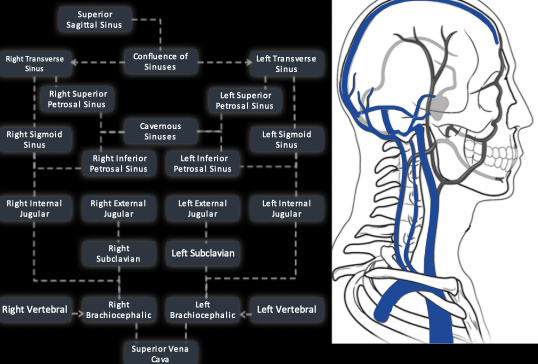
Venous Vasculature
Venous drainage does not follow the brain’s arteries. Instead they drain into the dural sinuses which drain into the internal jugular vein to the SVC.

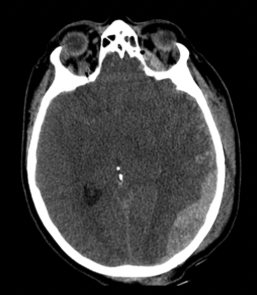
Common Pathologies: Hemorrhages
Hemorrhage can be seen as blood in spaces where it does not belong on imaging.
- Acute blood: bright white
- Subacute (older) blood: grey and eventually almost black once it is liquified (chronic state)
The type of intracranial hemorrhage is classified based on the anatomical location of the blood.
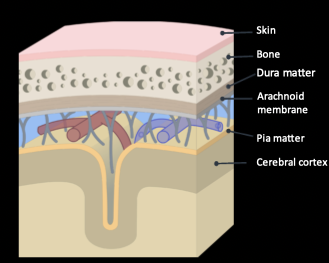
Scalp hematoma
- Between the scalp and the skin
- Clinically not concerning
Epidural
- Between the bone and the dura mater
- Source of bleeding is usually arterial, most commonly from a torn middle meningeal artery
- Usually caused by head trauma (possibly associated skull fracture)
- Imaging:
- Lentiform shape (biconvex)
- Can cross dural folds (midline)
- Does not cross cranial sutures
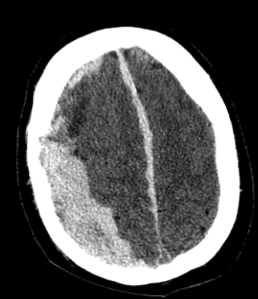
Subdural
- Between the dura mater and the arachnoid membrane
- Source of bleeding is typically venous, due to stretching and tearing of bridging cortical veins as they cross the subdural space to drain into dural sinus
- Imaging:
- Crescent shape hematoma
- Can cross cranial sutures
- Can fill dural folds but not cross (midline)
- Does not enter brain sulci (subarachnoid space)
- May have mass effect (shifting brain tissue away)
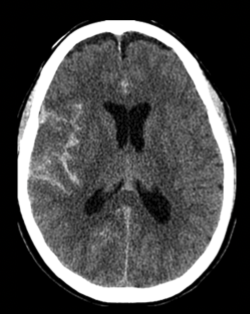
Subarachnoid
- In the subarachnoid space, between the arachnoid membrane and the pia mater
- Caused by trauma or rupture of intracranial aneurysm
- Presents with thunderclap headache
- Imaging:
- Blood fills subsrachnoid space which includes fissures, basal cisterns, and ventricles
- Blood is near rupture site when caused by aneurysm
- Note: due to the supine CT imaging position, blood may pool posteriorly; especially relevant if blood is only in ventricle which will be difficult to appreciate
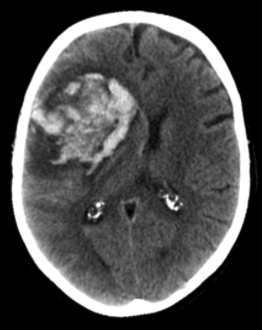
Intraparenchymal
- Bleed within the brain parenchyma
- Causes include trauma, tumour, hypertension, hemorrhagic conversion of a stroke, direct extension of other sources of bleeding
- Imaging:
- Blood seen in parenchyma
- Low density surrounding blood indicates cerebral edema
- Commonly associated with mass effect
- May appreciate underlying lesion (eg. tumour or aneurysm)
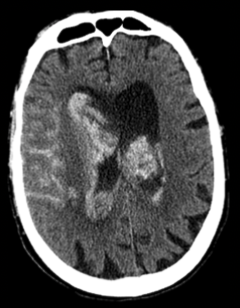
Intraventricular
- Bleed within the ventricles
- Causes include trauma, hemorrhagic tumour, direct extension from intraparenchymal hemorrhage
- Can result in acute hydrocephalus
- Imaging:
- Blood within ventricles
- Associated SAH or IPH
- Ventricles may be distended
Common Pathologies: Masses
Cerebral masses (tumours) can either be:
Intra-axial lesions
- Located inside the brain parenchyma
- Grey matter surrounds the mass (due to edema)
- Differential: primary brain neoplasms, metastasis, demyelinated disease, primary brain abscess/infection
Extra-axial lesions
- Located inside the skull but outside the brain parenchyma (ie. between and including the dura mater to the pia mater)
- Mass is directly adjacent to the skull; broad dural base may be seen with no brain matter between lesion and the dura
- May be surrounded by CSF
- Most common: meningiomas
Presence of multiple masses can suggest metastasis or brain abscesses.
Blood brain barrier:
- In normal patient, contrast will only be present in the blood vessels
- If there is damage to the BBB (eg. from tumour), IV contrast can pass through and cause enhancement of an intra-axial mass
Peripheral ring enhancement
This is a radiographic sign for abnormal findings when using radiocontrast.
- Glioblastoma: decreased density surrounded by bright rim; from BBB damage
- Metastases: may have peripheral ring enhancement or solid enhancement
- Brain abscess: can also have peripheral rim enhancement
Mass effects
As the intracranial space is fixed, any space-occupying lesion will increase intracranial pressure and displace the structures/soft tissue within the skull
- Midline shift: structures found in the midline are deviated to the contralateral side of the mass
- Ventricle effacement: edema surrounding the mass causes narrowing (effacement) of the ipsilateral ventricle
- Sulci effacement: mass causes the sulci on the ipsilateral side to efface
- Uncal herniation: uncus and adjacent part of the temporal lobe is pushed downwards compressing the brainstem and posterior cerebral arteries