creation date: 2026-02-09 18:48
status: note
tags: ACP Mental, Neurological & Musculoskeletal Health, Directed Independent Learning
MSK X-Ray Basics
Musculoskeletal X-ray - General Principles
Bone Anatomy
Zones
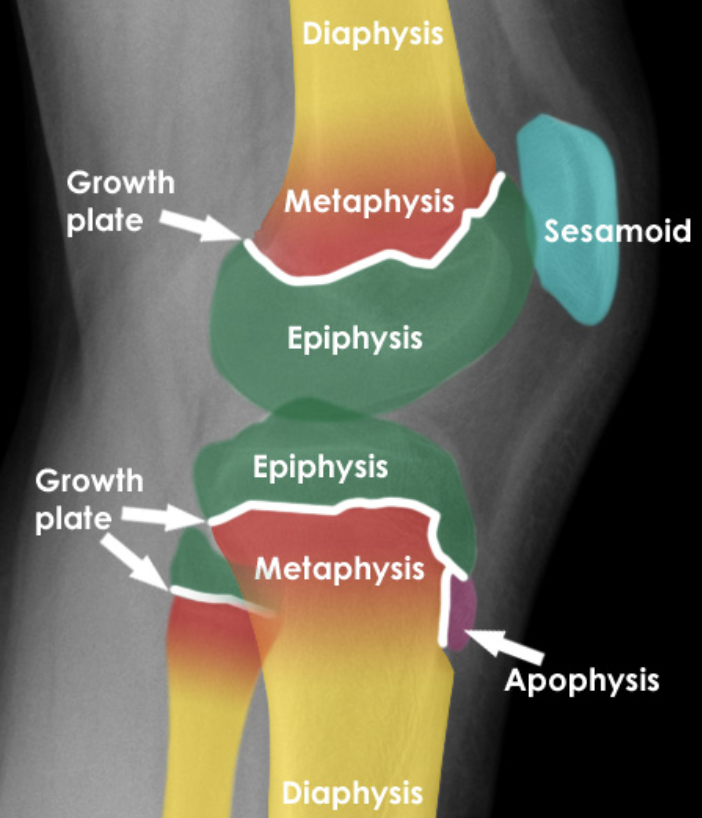
Most bones develop from cartilaginous ossification centres to form:
- Diaphysis (shaft)
- Epiphysis (End)
Growth plate separates diaphysis and epiphysis (epiphyseal line or physis). The zone adjacent to the growth plate on the diaphyseal side is called the metaphysis.
Sesamoid bone is a bone that ossifies within a tendon. Examples include:
- Patella
- At first MTP joint
- At first MCP joint
Apophysis is a normal developmental outgrowth of a bone that occurs from a separate ossification centre but fuses to the bone later.

Bone Structure
Bone consist of an outer cortex and inner medulla.
- Cortex: denser and thus whiter
Descriptions
Following fusing of skeleton, epiphysis, metaphysis, and diaphysis is less clinically important. As such less specific terms can be used to describe locations.
- Base, shaft, neck, head
- Proximal or distal
- Articular surfaces
Joint Anatomy
Most joints are:
- Synovial
- Contains two articulating bones
- Bones lined with hyaline cartilage and contained by a synovial lined capsule
Peri-articular soft tissues (ligaments and tendons) or cartilaginous structures may be visible on x-ray around joint
Narrowing of joint space implies abnormal thinning of cartilage
Systematic Approach
Approach consist of checking:
- Alignment of bone structures
- Joint spacing
- Integrity of bone cortex
- Medullary bone texture
- Abnormalities of visible surrounding soft tissue structures
Bone and joint alignment
Misalignment may be due to bone fracture or joint dislocation. There may be associated soft tissue injury that is not visualized.

- 3rd MTP joint dislocated
- Context: trauma
Joint spacing
Joint spacing may be:
- Narrowed due to cartilage loss
- Widened due to dislocation/dissociation

- Loss of joint space at 1st MTP joint that is more pronounced medially
- Context: OA (note osteophytes present too)
Cortical outline
The bone cortex (cortical outline is white lines) should be scrutinized for any breach of outline.

- Cortical outline abnormal
- Context: fractured ring finger metacarpal bone
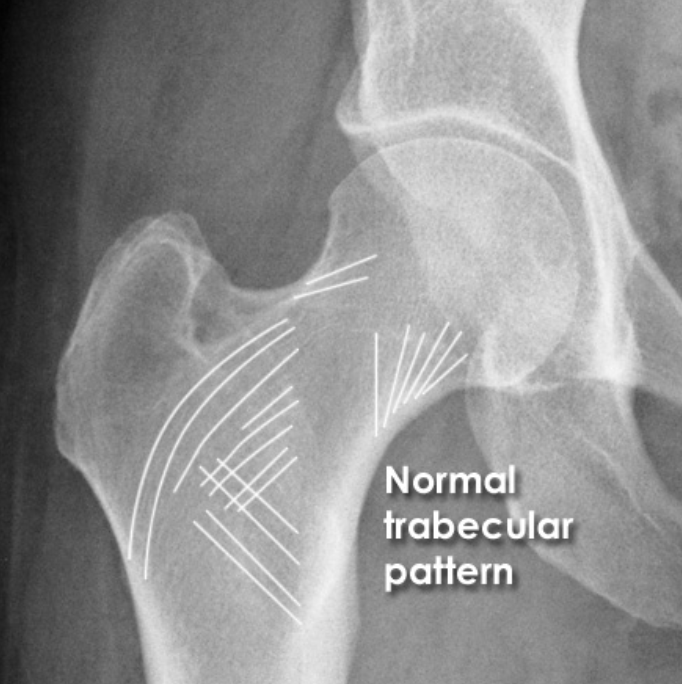
Bone texture
Fine matrix of fine white lines (trabeculae) can be seen with some bones. Bone injury or disease can result in abnormal texture.

Soft tissues
Surrounding soft tissue may provide additional information. Abnormalities include:
- Joint effusion containing fat and blood (lipohemarthrosis) that has leaded from bone following trauma
- Visible fracture line
Viewing Principles
In the context of trauma, at least two views of the body part are usually required. In other disease processes (eg. erosion from RA), one view may be sufficient.
While not routinely obtained, comparison to contralateral side may aid assessment. Additionally, comparison to past studies can improve diagnostic confidence.
Introduction to Trauma X-ray
Types of Fractures
The 4 classes of bones are long, short, flat, and irregular.
Long bone fractures
For long bones, fractures are described based on the direction of the fracture line relative to the direction of the bone shaft.
- Transverse: fracture is perpendicular to shaft
- Oblique: fracture is at an angle oblique to the shaft
- Spiral: fracture spirals along the shaft; due to twisting injury
- Sagittal plane: fracture passes longitudinally along the shaft
Irregular bone fractures
For short, flat, or irregular bones, description is determined by direction through the bone. In cases of multidirectional fracture, description may require greater detail.
Useful directional terms include: horizontal, vertical, coronal, sagittal, and axial.
Comminuted fractures
Injury that results in at least 2 separate bone components are comminuted. Some comminuted fractures have specific names.

Fracture Displacement
Displacement is defined by the position of the distal fracture fragment in relation to the proximal bone. Types of fracture displacements include:
- Angulation
- Rotation
- Change of bone length
- Loss of alignment
In most cases, fractures result in more than one type of displacement.
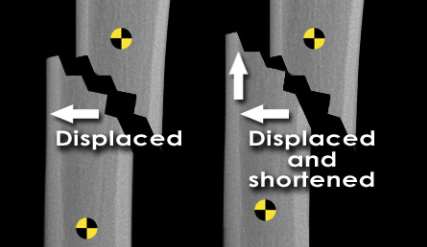
Loss of alignment (“displacement”)
Term can be used in a more specific context to describe the loss of alignment on the long axis (sideways movement).
Shortening
Describes proximal migration of the distal fracture component resulting in overall shortening of the bone length. Oblique fractures are more likely to be shortened (as it can “slide closer”)
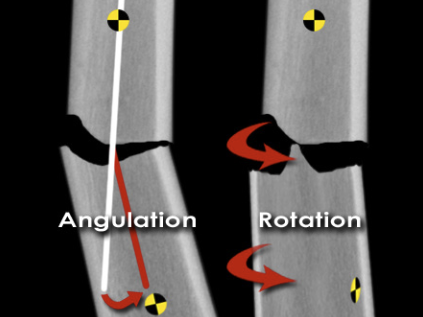
Angulation
Angulation is the degree of angle change of the distal component. Medial angulation can be termed varus, while lateral be termed valgus.
Rotation
Rotation of the fracture may be internal or external.
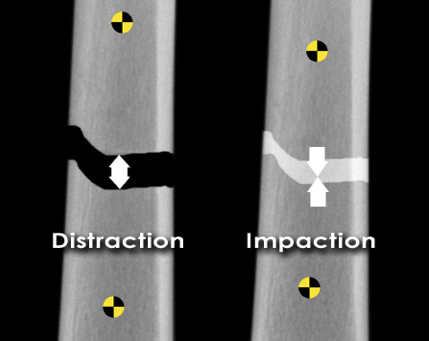
Distraction and impaction
A fracture resulting in increased overall bone length is due to distraction (widening) of the bone components.
If the bone shortens without loss if alignment, the fracture is impacted. This involves bone driving into each other.
Pathological Fractures
Fractures are terms pathological if the bone is abnormally weakened so that low impact trauma results in fractures (normal bone requires high force).
The most common cause of pathological fracture is osteoporosis. Other causes include bone tumours/malignancy.
Osteoporosis
Low bone density may be appreciated (compared to the cortical thickness of the normal bone). A subtle ulna fracture can be seen:

Multiple myeloma
Bone appears to be “moth-eaten”.

Bone lesions
A benign bone lesion can be at the site of fracture:

Other Fracture Types
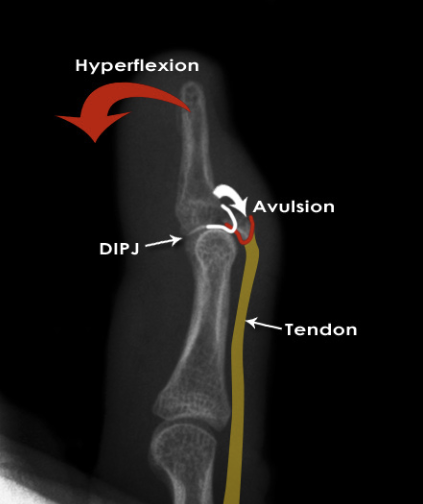
Avulsion
Bone/bone fragment is pull off (ie. avulsed) by a tendon or ligament due to excessive movement at a joint. Tendons/ligaments normally limit ROM but excessive force can move the bone while the tendon/ligament is still restraining.
A fracture that occurs due to this is referred to as an avulsion fracture.

Stress fracture
Repeated minor/low impact trauma to the normal bone can result in a fracture. This contrasts to pathological fracture as that would involve a single minor injury to an abnormal bone while stress fractures occur from repeated minor injury to normal bone.
March fracture: stress fracture of metatarsal from marching.
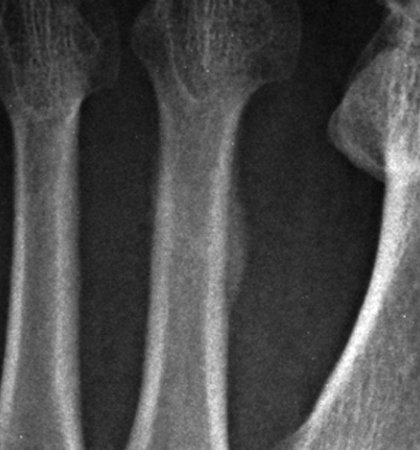
- Note: a fracture line is not visible but subtable calcification of the periosteum (periosteal reaction) suggests repeated trauma.
Periprosthetic fracture
A fracture occurring at the site of orthopedic metalwork.

- Lucent area around metalwork suggests loosening of prosthesis
- A fracture is seen through the weakened bone
Eponymous fractures
Eponymous fractures often have little consensus in criteria for diagnosis. As such, if there are any doubts to the nature/description of fracture, eponymous terms should be avoided.
Example: Colle’s fracture
Dislocation Injury
Dislocation results in the loss of anatomical congruence of bones at a joint. Similarly to fractures, dislocations are described in terms of the position of the distal bone in relation to the proximal bone.
The term subluxation may be used to describe an incomplete dislocation.
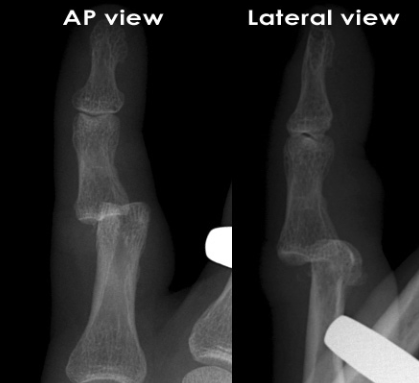
- Middle phalanx of the little finger
- Dislocated dorsally and laterally from the proximal phalanx
Fracture-dislocation
Fracturing of the bone with dislocation is termed fracture-dislocation.
Diastasis
Refers to the separation of 2 normally adjacent bones that is normally held together at a ligamentous joint or growth plate (eg. pubic bones at the pubic symphysis)
Management
Treatment
In all cases, appropriate resuscitation and care should be done.
Treatment usually consist of:
- Reduction - to return bone to an anatomical position
- Immobilization - for long term healing
Immobilization
Several materials can be used for immobilization.
- Strapping: bone is held in the correct position by strapping it to another nearby bone (eg. wrapping pinky toe to 4th toe)
- Plaster cast
- Kirschner wires (K-wires): wires placed through skin under anesthesia
Reduction
Completed prior to immobilization so healing can proceed correctly. Reductions may occur through external manipulation. However, if that is not successful or not appropriate, open reduction and surgical immobilization may be required.
- Open reduction and internal fixation (ORIF)
- Interno-external fixation frame
- Bone grafting
Complications
Bone fractures can be complicated by significant soft tissue injury that may not show up on x-ray. It is important to check for neurological and vascular compromise prior to x-rays.
- Open fracture: fracture complicated by breach in adjacent skin
- Closed fracture: no break in skin; closed fractures that are complicated by soft tissue injury are termed “complex fracture”
Complications include:
- Malunion: if a fracture heals in an abnormal position
- Non-union: bone does not reconnect with healing
- Avascular necrosis (AVN): bone does not heal due to internal blood supply compromise
- Osteopenia and Sudeck’s atrophy: prolonged immobilization may result in osteopenia and reduced bone density
Fracture Mimics
A number of anatomical features may mimic fractures on x-ray.
- Growth plates
- Unfused apophysis
- Accessory ossicles
- Vascular/nutrient lines (low density black lines through the cortex usually)
- Harris lines (sclerotic lines transverse)
Foreign Bodies
Foreign bodies may be present following traumatic breach of the skin. X-ray is helpful for radiopaque materials such as glass or metal but other less dense materials such as wood are not as easily detected.