creation date: 2024-12-24 19:12
modification date: Tuesday, December 24th, 2024 19:12:27
status: note
tags:
Electrocardiogram
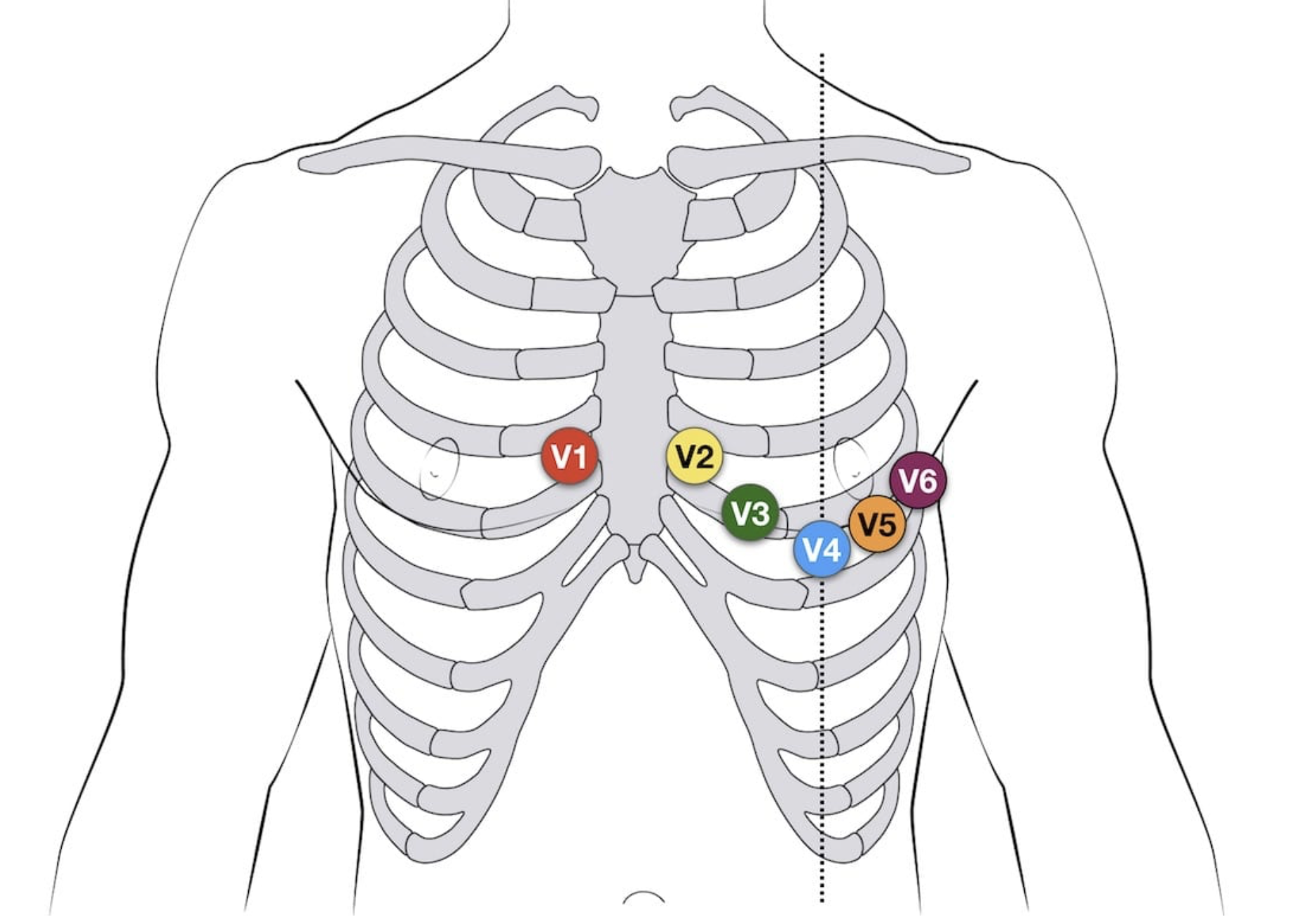
Lead placement
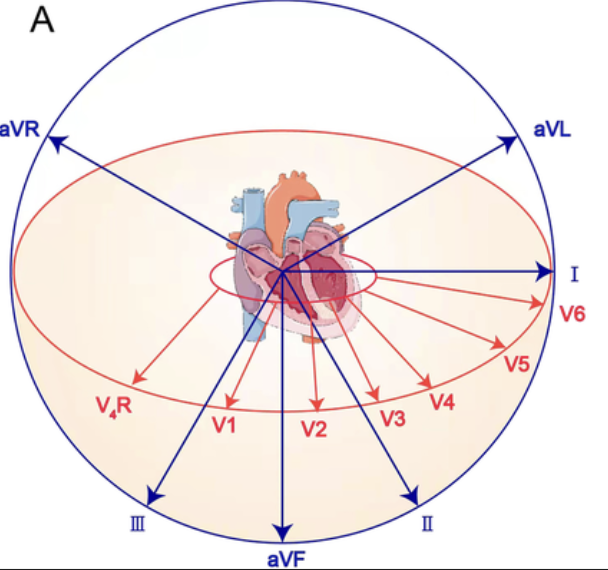
Views
II, III, aVF:
- Inferior
- Right coronary artery, marginal branch
I, aVL, V5, V6: - Lateral
- Left coronary, circumflex & obtuse marginal
V1, V2: - Septum
- Left coronary, septal branch
V3, V4: - Anterior
- Left coronary, anterior descending, diagonal arteries
Normal values
ECG settings: 25mm/sec, 10mm/mV
Rhythm: regular P-P, R-R if ±0.06s (1.5 small box)
Heart rate:
- If regular: 1500 / # small boxes
- If irregular: # of complexes in 6 sec * 10
P-wave morphology: rounded and upright
Q-wave is < 1/3 of R wave, <0.04s
PR interval: 0.12-0.20s (3-4 small boxes)
QRS: 0.06-0.10s (1.5-2.5 small boxes)
Note: fastest electrical impulse dictates heart rate - normally SA node
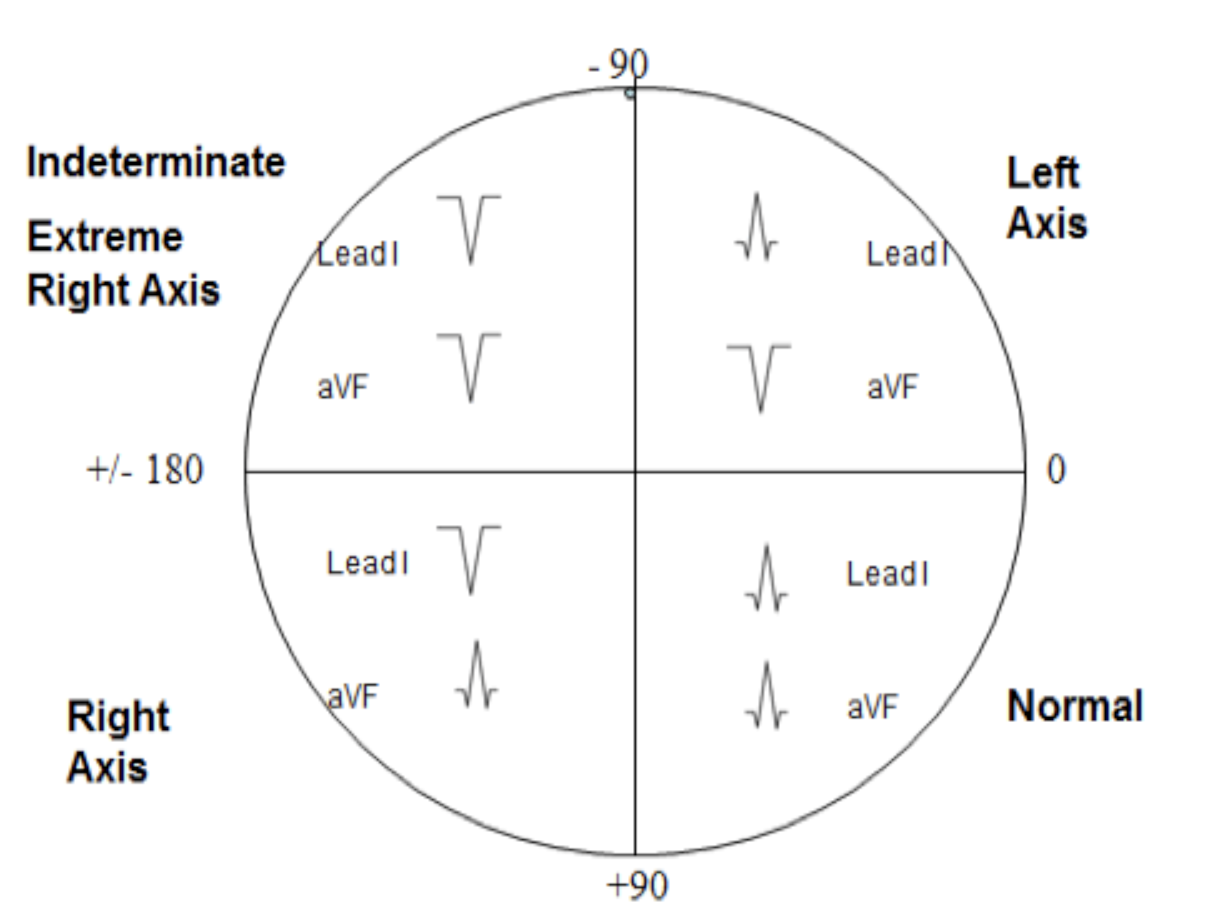
Axis
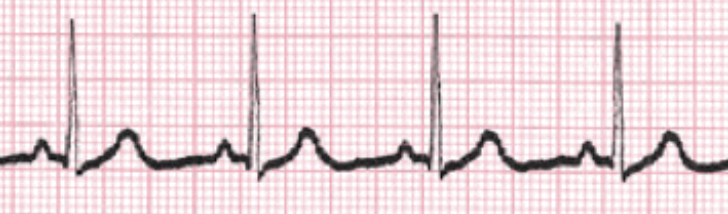
Sinus Rhythms
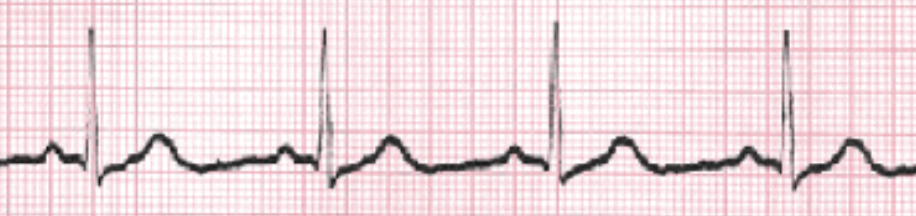
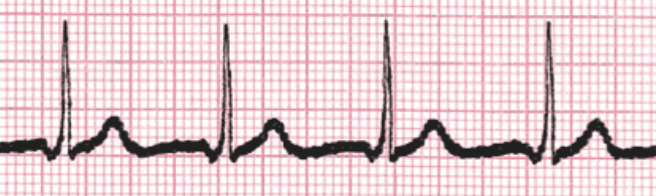
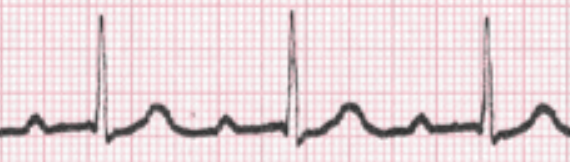
Sinus Rhythm (Normal)
- HR: 60-100bpm
- P wave for every QRS
- See Normal values above
Sinus Bradycardia
- HR < 60bpm
- All else normal
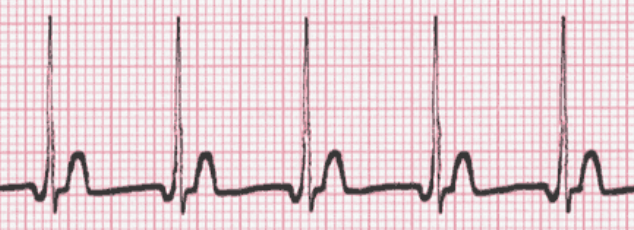
Sinus Tachycardia
- HR > 100bpm
- Complexes may come together, partially burying P waves

Sinus Dysrhythmia
- Irregular rhythm (changing HR), can coincide with breathing
- All else normal
- Pathophysiology: from parasympathetic response (eg. from vagus nerve pressure) - can be from breathing, medication, etc.

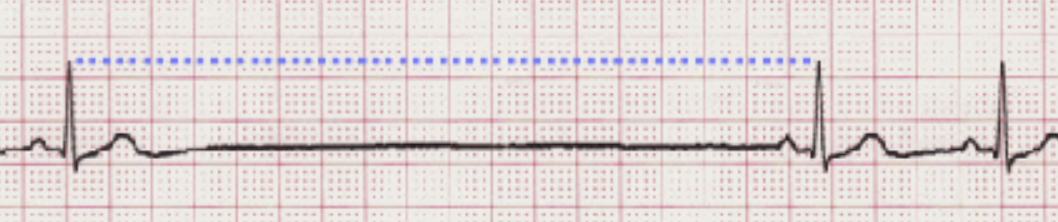
Sinus Arrest
- Pause in activity, typically constant R-R interval prior
- Pause >6s is emergency
- Pathophysiology: SA node stopped
Sinus Exit Block
- Same as sinus arrest EXCEPT pause duration is multiple of R-R interval

Atrial Rhythms
Premature Atrial Complex
- Change in P wave morphology but upright
- Can occur frequently or occasionally
- Pathophysiology: Early impulse occurs in atria other than SA node
Wandering Atrial Pacemaker
- Three differently shaped P waves
- Rhythm may or may not be regular
- Pathophysiology: Location of impulse source moves/wanders in atria

Multifocal Atrial Tachycardia
- Same as wandering atrial pacemaker EXCEPT HR > 100 bpm
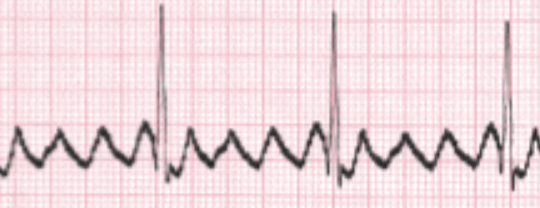
Atrial Flutter (Aflutter)
- Atrial depolarization denoted by series of “F” waves (no P wave)
- Flutter rhythm documented with F:QRS ratio
- Pathophysiology: Obstruction within atrial conduction causing series of rapid depolarization; AV node blocks extra impulses
Atrial Fibrillation (Afib)
- Atrial activity denoted with “f” waves (no P waves)
- f waves can be coarse (≥3mm) or fine (<3mm)
- Irregular R-R interval
- HR often >160bpm
- Pathophysiology: Multiple impulses occur within atria (chaotic); AV node overwhelmed by chaotic electrical activity; HR high due to loss of cardiac output due to “quivering” atria
Junctional Rhythms
- Impulses initiated in AV junction; affects P wave morphology based on locatino of impulse
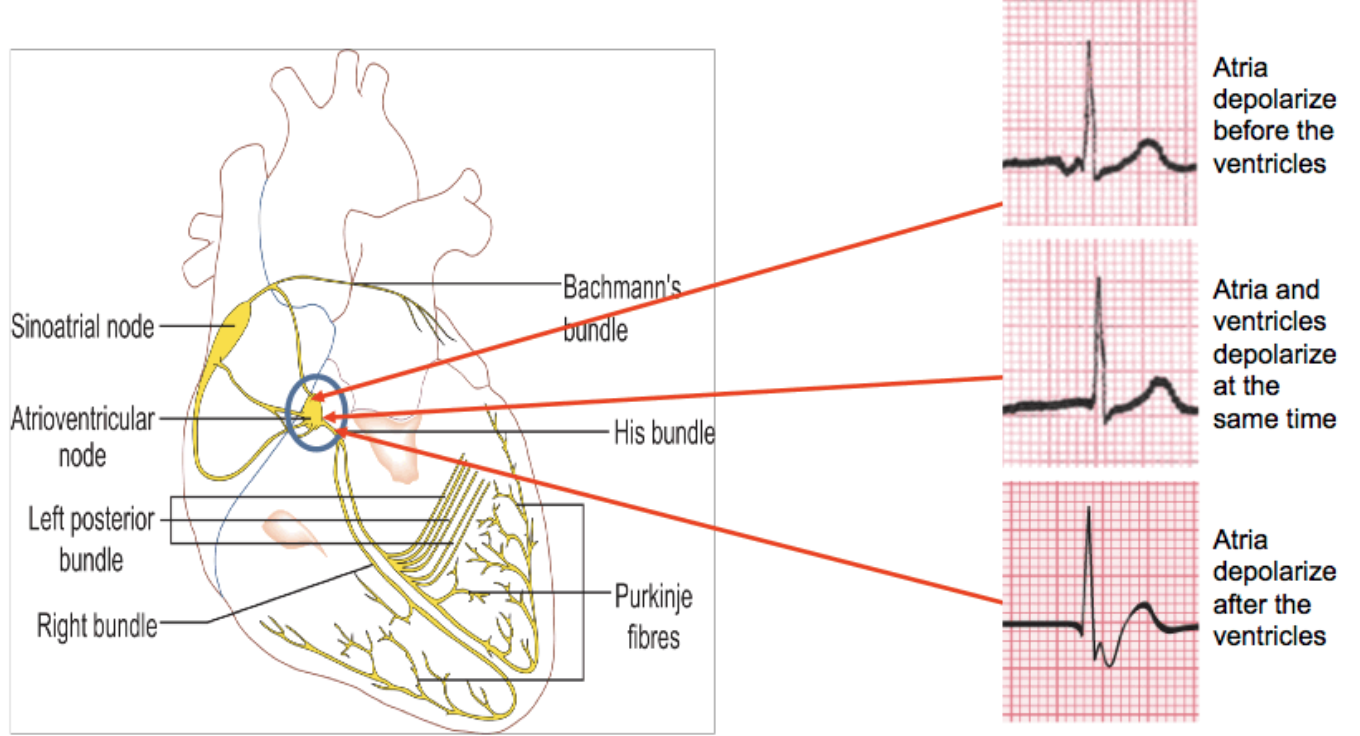
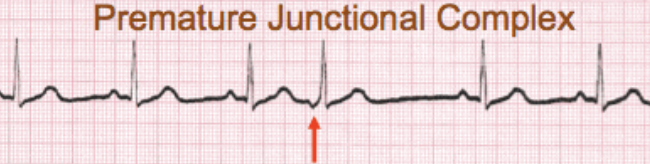
Premature Junctional Complex (PJC)
- Abnormal P wave (see above)
- Often occur in bradycardic rhythms
- Disrupts underlying rhythm by occurring early
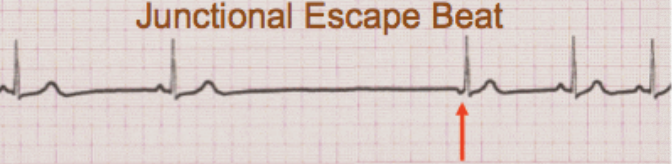
Junctional Escape Beat
- Same morphologically as PJC
- Often terminate sinus arrest
- Pathophysiology: SA impulses too slow, junction acts as backup pacemaker
Junctional (Escape) Rhythm
- Atrial activity due to AV junction
- HR 40-60bpm (AV junction rhythm)
- See above for P wave morphology
- If P wave before QrS, likely shorter than normal (<0.12s)
- P wave can also be buried or occur after QRS

Accelerated Junctional Rhythm
- Same as junctional escape rhythm except HR 60-100 bpm
Junctional Tachycardia
- Same as Junctional escape rhythm except HR 100-180 bpm
Supraventricular Tachycardia (SVT)
- Impulses above ventricles (ie. AV node or above) with HR 150+ bpm
- Overlap of P wave and previous T wave

Ventricular Rhythms
- Pathophysiology: Failure of faster pacemakers in heart or abnormal stimulation of ventricle resulting in faster rate of ventricular impulse
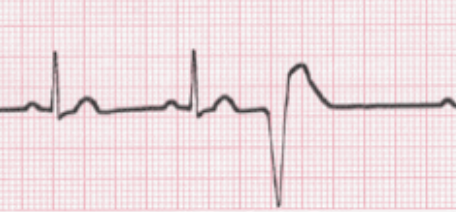
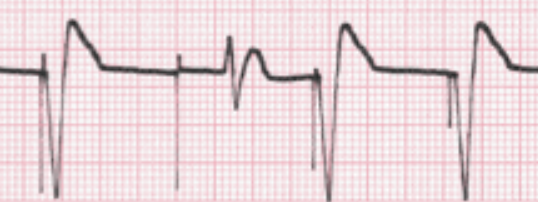
Premature Ventricular Complexes (PVC)
- Early impulse from ventricle disrupts underlying rhythm
- Absence of P wave and wide, bizarre QRS
Agonal Rhythm
- HR < 20 bpm
- No P waves and wide, bizarre QRS
- Regular or irregular rhythm often indeterminable due to slow rate

Idioventricular Rhythm
- HR 20-40 bpm
- No P waves and wide, bizarre QRS

Accelerated Idioventricular Rhythm
- HR 40-100 bpm
- No P wave and wide, bizarre QRS
Ventricular Tachycardia (VTach)
- HR >100 bpm
- No P wave and wide, bizarre QRS
- Can treat with defibrillation

Ventricular Fibrillation (VFib)
- No P wave, no QRS
- Heart is not beating
- Pathophysiology: Small regions of tissue are independently depolarizing causing heart to “quiver”

Asystole
- Total absence of electrical activity
- Clinically dead

Ventricular Asystole
- Asystole except P waves still present
- Clinically dead

Pacemaker Rhythms
Atrial Pacemaker Rhythm
- Pacing spike immediately preceding P wave
- PR interval is from spike to QRS
Ventricular Pacemaker Rhythm
- Pacing spike immediately preceding the QRS complex
- May or may not have P waves

Atrioventricular Pacemaker Rhythm
- Pacing spike immediately preceding P waves and QRS
- PR is atrial spike to ventricular spike - referred to as AV delay, programmed by physician
Failure (Loss) to Capture
- Presence of pacing spike but no waveform immediately following it
- Inherent rhythm becomes present
Heart Block
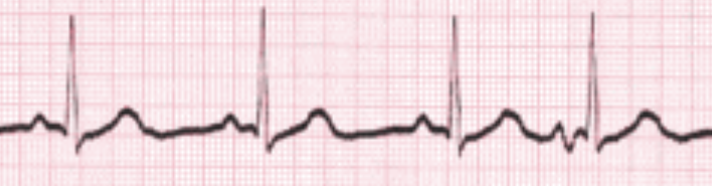
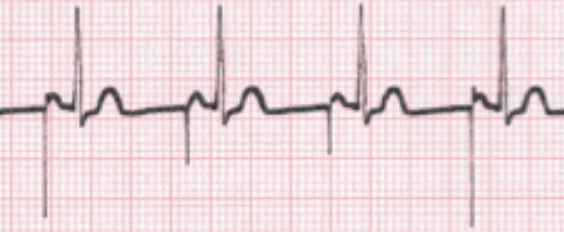
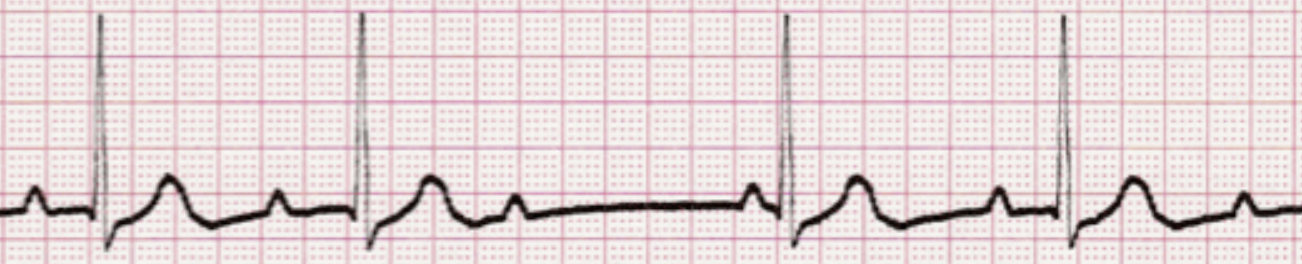
First Degree Heart Block
- Looks like sinus rhythm EXCEPT P-R interval regular and >0.20s (4 small box)
- Typically stable; if occur during MI, should monitor
Second Degree (Mobitz) Heart Block Type I
- Aka Wenckebach Phenomenon
- Prolonging P-R interval from one complex to the next until QRS is non-conducted, pattern then restarts
- P-P intervals are regular, R-R interval irregular
- Typically stable/temporary as long as ventricular response remains “normal”
Second Degree (Mobitz) Heart Block Type II
- Constant P-R interval with missing QRS
- QRS can occur in specific ratio to P waves OR unpredictable
- Can progress to third degree heart block

- (3:1 block)
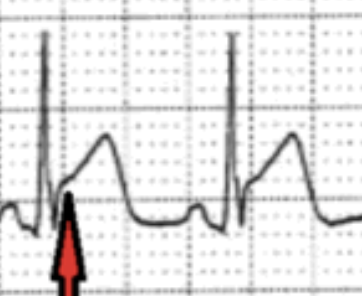
Third Degree Heart Block
- Aka Complete Heart Block
- Regularly occurring P waves and QRS complexes at two distinct rates
- Pathophysiology: Disease or tissue death preventing atrial impulses from entering ventricular conduction system

- (Red arrow pointing to buried P wave)
Bundle Branch Block
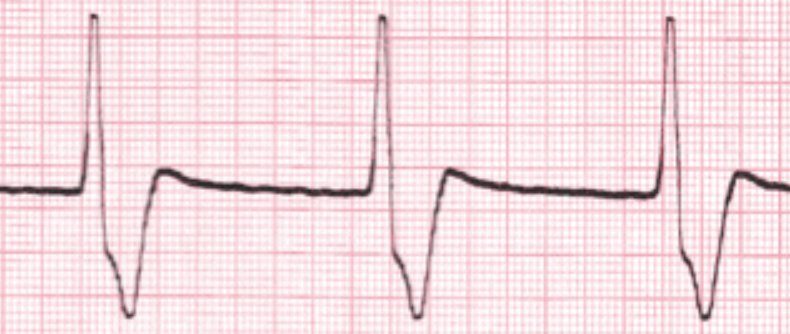
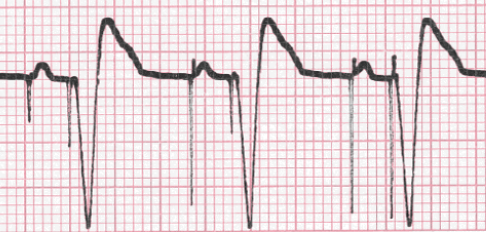
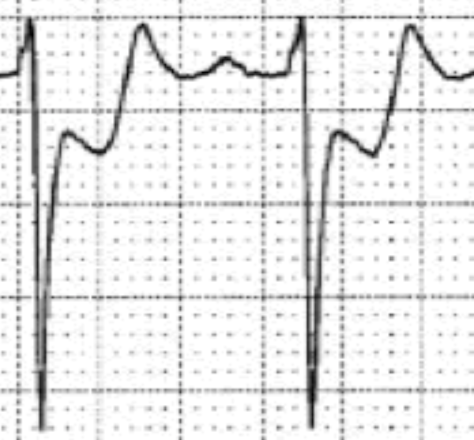
Left Bundle Branch Block (LBBB)
- Widen QRS (>0.12s; 3 small box)
- Dominant S wave in V1 (points down)
- Broad monophasic R wave and absence Q wave in lateral leads (I, aVL, V5-6)
- Prolonged R wave peak in leads V5-6

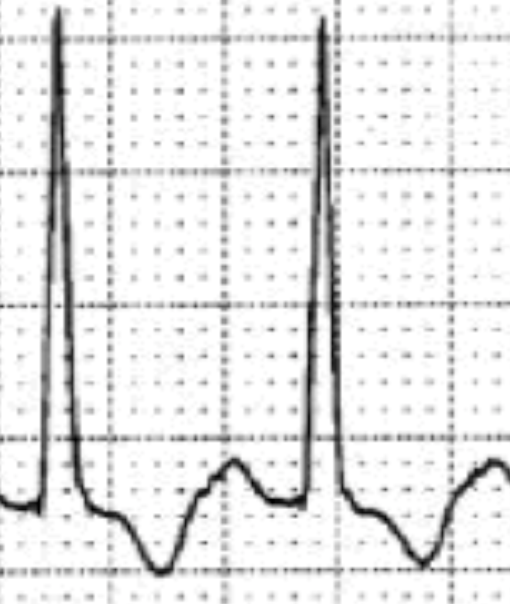
Right Bundle Branch Block (RBBB)
- Widen QRS (>0.12s; 3 small box)
- RSR’ in V1-3 (M-shaped QRS)
- V1 points up
- Wide, slurred S wave in lateral leads (I, aVL, V5-6)

Fascicular Blocks
Left Anterior Fascicular Block (LAFB)
- Left axis deviation (positive in lead I, negative in aVF)
- qR complex in lead I, aVL
- rS complexes in lead II, III, aVF
- May have prolonged QRS, increased QRS voltage in limb leads
- Ex: LITFL
Left Posterior Fascicular Block (LPFB)
Ventricular Hypertrophy
Left Ventricular Hypertrophy
- S wave depth of V1 + tallest R wave height in V5 or V6 is > 35mm
- Should find evidence of left ventricular strain (ST depression or T wave inversion in left-sided leads)
- Pathophysiology: Thickened LV wall results in prolonged depolarization (R wave peak time) and delayed repolarization (strain indicators)
Right Ventricular Hypertrophy
Ischemia, Injury, Infarction
- Look for changes in anatomically contiguous leads (eg. II, III, aVF), should show up in more than one
Ischemia
- Delay in repolarization resulting in:
- ST segment depression of ≥1 mm
- T wave inversion in two or more anatomically contiguous leads
| ST depression | T inversion |
|---|---|
 |  |
Injury
- Delayed ischemia for few minutes can worsen to myocardial injury
- ST segment elevation of ≥1 mm in two or more anatomically contiguous leads
Infarction
- ST elevation, T wave inversion during MI
- Following MI, ST and T returns to normal but Q wave will remain increase duration (≥0.04s) or depth (≥ 1/3 height R wave)