creation date: 2025-09-11 16:23
tags: Pathologies Incomplete
Tuberculosis
Background
Definitions
Tuberculosis (TB) is a highly prevalent and potentially fatal infection that predominantly affect regions that are poor, overcrowded, and lacking in public health infrastructure.
TB is a preventable disease but due to the difficulties in detection and the challenging treatment regime, TB continues to infect significantly worldwide.
Latent tuberculosis refers to an infection in which bacteria are alive but contained by the host immune system resulting in no clinical manifestation or evidence of infection. There is also no risk of transmission.
Active tuberculosis refers to an infection in which the bacteria is actively multiplying, causing tissue damage, and inflammation. This manifests in the symptoms of TB.
Reactivation tuberculosis refers to occurrence of TB symptoms after a period of latency. The risk of reactivation for a healthy adult is 5% in the 2-5 years following infection and another 5% in all subsequent years after that.
Miliary tuberculosis (systemic) refers to extra-pulmonary involvement in which TB is spread to the kidneys, meninges, lumbar vertebrae, adrenal glands, liver, cervical lymph nodes, joints, and long bones.
Microbiology
Tuberculosis arises from an infection from a group of bacteria known as the Mycobacterium tuberculosis complex. Mycobacterium tuberculosis is the predominant cause of TB in humans but M. bovis, M. africanum, and M. canetii can also infect humans.
Mycobacterium have a number of characteristics that increases their virulence:
- Cell wall and envelope - strong barrier to antibiotics
- Slow growth rate (generation time approximately 20-24 hours) - difficult to detect by culture
Pathophysiology
Tuberculosis bacilli are spread typically via airborne droplets which can remain suspended in the air for several hour. The likelihood of infection increases with exposure time to droplets in an enclosed space. Rarer forms of contraction is through ingestion of contaminated milk and through contacts with droplets on nonintact skin.
Once inhaled, the droplet must make it to the alveoli where infection may be established. In many cases, droplets land on the upper airway mucosa where infection is unlikely to take place.
The mechanisms responsible for the containment and reactivation of the infection is poorly understood. A number of virulence factors aid M. tuberculosis in survival outside and within the host:
- Cell wall components which circumvent desiccation to allow for suspended droplet form
- Ability to survive within antigen-presenting cells, airway cells, and more by preventing phagosomal maturation (and thus remaining phagocytosed without dying)
- Ability to manipulate cell death pathways to allow for phagosomal escape and transmission
- Ability to remain dormant via granuloma formation (type IV immune response) - allows for reactivation up to decades later
- Dissemination within the host via direct spread through tissue destruction, distant spread through lymphatics or blood (likely through antigen presenting cells)
- Immune system manipulation to reduce immune responses and inflammation
- Ability to escape into airways and aerosolized for host-to-host transmission
- Ability to induce cough reflex which increases aerosolization
A number of other mechanisms and interactions may also be present based on lineage (M. tuberculosis has 7 distinct lineages) and host factors.
In an immunocompetent person, innate and adaptive defences are typically sufficient in maintaining TB in a latent state:
- Recognition of M. tuberculosis by toll-like receptors
- Direct/indirect killing via reactive nitrogen intermediates
- Cytokines and cytotoxic granules
- Granuloma formation - necrosis inside with T-helper cells and macrophages outside to form Ghon complex; once fibrosis occurs on the outside, this becomes ranke complexes
- T-cells (against dessiminated TB)
- Humoral immunity
In cases were host immunity is insufficient, the granulomas can erode into the airway forming cavities. Areas of cavitation:
- Promotes development of drug resistance
- No longer carry out respiratory function
- Allow for opportunistic bacteria and fungi growth
- Adjacent lung parachyma becomes fibrotic
- Pulmonary vessels may erode
This results in the clinical manifestations of TB.
Clinical Presentation
Signs & Symptoms
Patients with latent TB are asymptomatic which may carry into early active TB.
As TB progresses, symptoms often appear insidiously:
- Cough
- Fever
- Night sweats
- Weight loss
- Hemoptysis
Symptoms are generally nonspecific and is easy to miss if TB is uncommon in the clinician’s region.
Miliary tuberculosis may manifest with end-organ findings associated with points of spread. This is more likely with reactivation TB.
History & Physical Exam
History should elicit:
- Prior TB status
- Known contacts of exposure
- Country of origin
- Foreign travel
- Family history
- Occupational/residential exposures
- Immunosuppression/immunocompromised status
Physical findings may find:
- Areas of consolidation
- Airway inflammation
- Cavities
- Chest wall deformities (if chronic)
Physical findings can be very broad, involving any organ, due to extrapulmonary TB involvement.
Risk factors
Risk factors for developing active tuberculosis are:
- Immunocompromised state
- Tobacco use
- Excessive alcohol use
Risk factors for contracting TB are:
- Tight living quarters
- Below or at poverty lines
- Refugee/immigrant
- Immune system issues
- Substance abuse
- Kids (<5 years of age)
- Occupational: healthcare, mining, prisons, shelter
Diagnosis
Criteria
Diagnosis can be challenging due to the variety of manifestations and nonspecific nature of the symptoms and signs. Criteria for diagnosis depends on whether the patient is being evaluated for latent, active pulmonary, or extrapulmonary tuberculosis.
Latent tuberculosis
A number of options are available for screening:
- Mantoux (2-step skin test)
- IGRA (more specific, but costly)
It should be noted that some tests (eg. Mantoux) have false-negative results often when they are done shortly after infection or if immunocompromised.
It is also important to note that some tests cannot distinguish between active or latent disease and thus active TB should be ruled out prior to treatment for latent TB.
Active tuberculosis
Gold standard of diagnosis is by isolation of M. tuberculosis from bodily secretion or fluid (eg. sputum, bronchoalveolar lavage, or pleural fluid) or tissue (eg. pleural/lung biopsy):
- Sputum culture (true standard, but takes 12 weeks)
- Acid-fast bacilli smear
- Molecular detection via NAATs and lateral flow biomarker detection
Diagnosis is sometimes made presumptively based on supporting evidence if a fluid sample is not available. This includes:
- Clinical history
- Imaging (CXR, CT if needed)
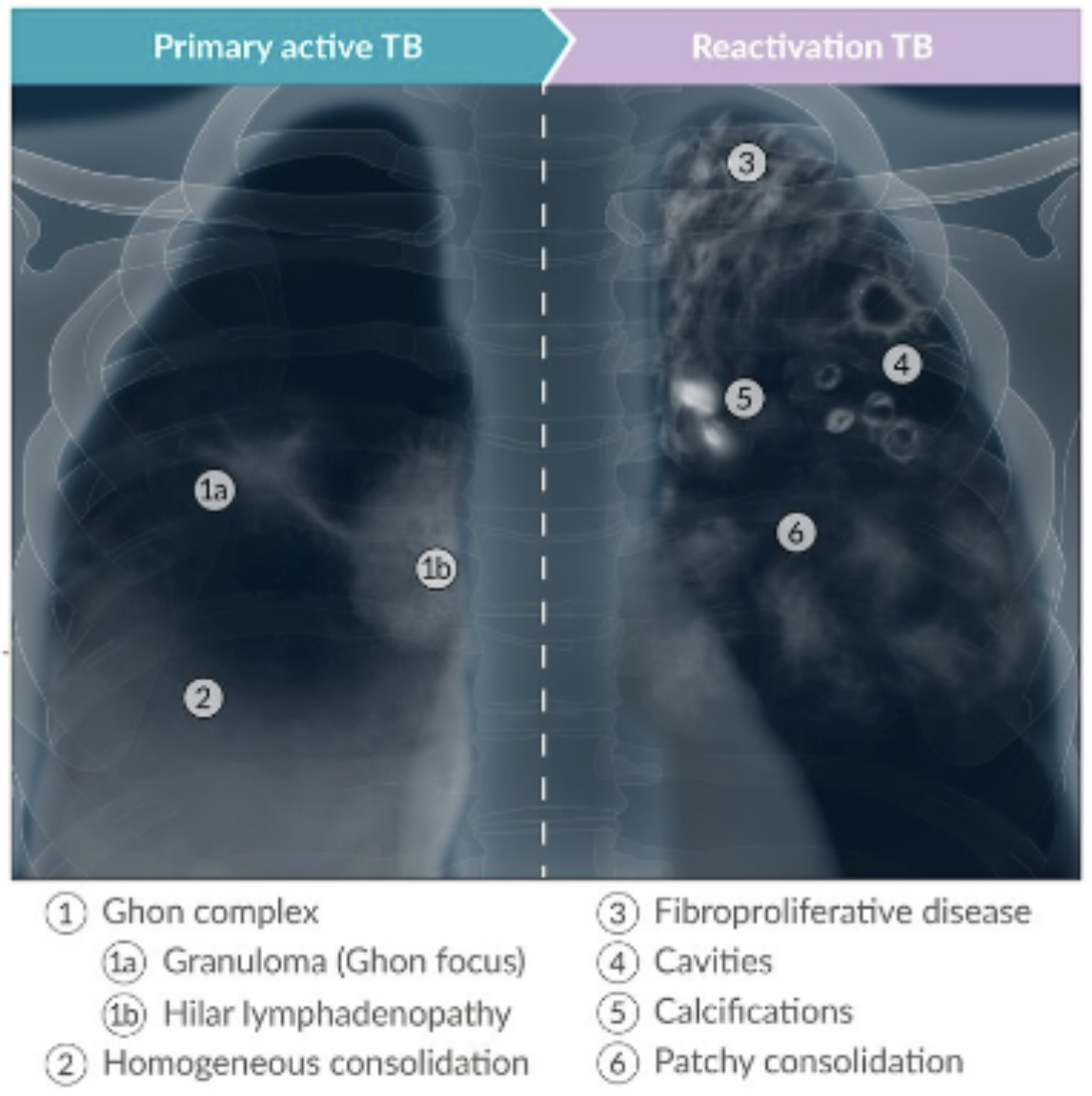
- Upper lobe or superior segment lower lobe infiltrates, cavitations, consolidation (note: superior segments of lung affected because of relatively higher oxygen tension, lower lymphatic flow, reduced blood perfusionl; also less breathing amplitude so lesions may remain)
- Hilar or mediastinal lymphadenopathy
- Pleural effusion
- Miliary node
- CT, MRI, PET-CT can define anatomic involvement
CXR findings
Work-up
Screening for latent tuberculosis
Screening is recommended for the following populations:
- People with HIV
- Household or close contact with individual with active TB
- Patients initiating immunosuppressants
- Dialysis patients with end-stage renal disease
- Patients with silicosis or history of occupational silica exposure
- Populations in areas with estimated TB prevalence of 0.5% or higher (eg. sub-saharan Africa, southeast Asia, parts of the western Pacific)
- Patients in subpopulations experiencing structural risk factors for TB (eg. unhoused)
When screening, consider the factor for why the test could be falsely-positive. If sufficient, consider starting with a chest x-ray which may allow for quicker management.
A chest x-ray is used to rule out asymptomatic active TB.
Suspected active TB
Following suspicion of tuberculosis based on history, physical, and risk factor assessments, patients should undergo chest radiography followed by three sputum specimens (8 hour apart including at least 1 early-morning specimen).
In immunocompromised patients (incl. HIV patients), mycobacterial cultures of blood and urine should be performed.
Differential
Diagnoses to not miss are:
- Pulmonary embolism with infarction - CT pulmonary angiography
- Pneumocystis jirovecii pneumonia - PCR of samples
- Diffuse alveolar hemorrhage from vasculitis - serology
Other possible diagnoses which present similarly to TB include:
- Community-Acquired Pneumonia
- Nontuberculous mycobacterial pulmonary disease
- Endemic fungal pneuamonias
- Sarcoidosis
- Primary lung carcinoma
- Silicosis or other pneumoconioses
Red Flags / Complications
A number of complications can result, many of which have poor health outcomes. Complications occur more commonly in settings of reactivation disease.
- Hemoptysis
- Pneumothorax
- Bronchiectasis
- Extensive pulmonary destruction
- Fistula
- Tracheobronchial stenosis
- Malignancy
- Chronic pulmonary aspergillosis
Management
Prevention
BCG vaccination can be used for primary prevention. This is more effective in children compared to adults.
Treatment of latent tuberculosis
Once active TB is ruled out, treatment of latent TB can reduce the risk of progression to active TB.
A number of regimens are available with equal efficacy. Selection is based on the likelihood of adherence, potential for adverse effects, and preferences.
Generally preferred are rifamycin-based:
- Rifampin daily for 4 months (4R)
- Isoniazid and rifampin daily for 3 months (less preferred with older age)
It is important treatment is monitored monthly for side effects and symptoms of hepatitis.
Treatment of pulmonary tuberculosis
Drug-susceptible TB in nonpregnant adults without HIV
Treatment consist of a traditional regimen or a shortened regimen. The traditional regimen is the standard of care but the shorten regimen may be considered should they meet the criteria.
It is recommended to ensure adherence and safety, and to prevent drug resistance by having the medication be taken under supervision of a healthcare provider.
Traditional regimen
This regimen lasts 6 months. It begins with a two month intensive phase of the “RIPE therapy”:
- Rifampin (RIF)
- Isoniazid (INH)
- Pyrazinamide (PZA)
- Ethambutol (EMB)
followed by a continuation phase of: - RIF
- INH
for at least 4 additional months. During the continuation phase, assessment should be made two months should be made based on chest radiograph and sputum AFB culture which determines the approach to completing treatment.
Note that dosing is based on weight. PZA can be excluded based on side effects but doing so will extend the continuation phase to seven months.
Note that due to adverse effects, patients must not drink alcohol (RIF),
Shortened regimen
This regimen is rifapentine-moxifloacin-based and lasts 4 months. It consists of and 8 week intensive phase of daily:
- Rifapentine
- Isoniazid (INH)
- Pyrazinamide (PZA)
- Moxifloxacin
followed by a 9 week continuation phase of daily: - Rifapentine
- INH
- Moxifloxacin
The criteria for this regimen requires the patient:
- Has no suspected or confirmed resistance to the medication
- Has no history of cardiac morbidities
- Does not have liver disease, renal insufficiency, and/or laboratory abnormalities
- Is not pregnant or lactating
- Is not on medication that may interact
- Is unwilling or unable to afford, assess, or take on the increased pill burden associated with the regimen