creation date: 2025-07-06 17:00
tags: Pathologies
Osteoarthritis
Background
Definitions
Osteoarthritis is an inflammatory condition of the joints that result in articular changes/loss resulting in chronic pain. It is one of the most common cause of chronic disability.
A number of structures are involved including the subchondral bone, synovium, and periarticular structures. Environmental and psychosocial factors, as well as pain pathway changes affect the chronic aspects of the pain.
Etiology and Pathogenesis
Historically, OA has been attributed to degeneration associated with “wear and tear”. However, the development of OA is complex and also consist of inflammatory processes.
Inflammatory changes
Classic cellular inflammation that results in elevated leukocytes in the affected joint tissue and synovial fluid is typically not prominent in OA, rarely exceeding 1000-2000 cells/mL. This is in contrast with rheumatoid arthritis which will have synovial fluid leukocytes exceed 2000 commonly.
However, in some cases, synovial inflammation of OA may be comparable to RA but differ in that OA is macrophage dominant while RA is more T and B cell dominant.
Proinflammatory factors drive the production of proteolytic enzymes which degrade the extracellular matrix resulting in joint tissue destruction. It is unclear the level of contribution proinflammatory factors and mechanical factors play in the development of OA. There may also be interplay involving the stimulation of proinflammatory factors due to mechanical wear and joint loading.
Anatomic/physiologic changes
OA can be described as the result of a joint’s inability to repair itself following insult. With exception of post-traumatic OA, which starts with an acute injury to specific tissue, the exact joint tissue that is affected first is hard to determine.
Articular cartilage:
- Normally provides smooth, low-friction surface for joint motion
- Requires hyaluronic acid, which requires presence of lubricin aka proteoglycan-4, in synovial fluid to provide viscosity
- Chondrocytes which are the only cells in cartilage are typically dormant
- OA change:
- Collagen network loosens and allows hydrophilic proteoglycans to attract water causing cartilage swelling
- Chondrocytes proliferate due to loss of matrix causing hypertrophic chondrocytes producing type X collagen and MMP-13
- Over time chondrocyte die off as matrix continue to be damaged and repair becomes limited
Bone:
- Joint remodeling occurs to stabilize the joint in response to abnormal mechanical loads
- Subchondral bone thicken due to increased collagen production that is improperly mineralized
- Osteophytes form at joint margins, often at tendon or ligament insertion sites
- Bone cyst may also occur but erosions are rare
Synovium: - Some degree of synovial inflammation and/or hypertrophy is expected with symptomatic OA
- Not thought of to be an initiating factor of OA
- Predominantly macrophages in fluid and contributes to pain
Soft tissue: - Ligaments, joint capsule, menisci extracellular matrix disruption and cell loss
- Tears are common with long-term OA which can further cause inflammation
Risk factors
Multiple risk factors are linked to pathogenesis of OA:
- Age - thinning of artilage, reduced hydration, accumulation of proteins
- Joint injury - usually develops within 10 years of injury causing inflammation
- Obesity - excess weight produces increased load; possible metabolic component
- Genetics - mutations in structural collagens can result in premature OA
- Anatomical factors - joint shape, esp. the hip can cause premature OA
Clinical Presentation
Signs & Symptoms
The primary symptoms of OA are joint pain, stiffness, and locomotor restriction. Symptoms are usually present in one or few joints.
Pain
- Associated with joint use and relieved by rest
- Stage 1: predictable, sharp pain following mechanical insult
- Stage 2: constant and affect daily activities; unpredictable episodes of stiffness
- Stage 3: constant dull/aching pain punctuated by episodes of unpredictable, intense, exhausting pain resulting in severe limitations in function
Tenderness - Joint-line suggests articular
- Non-joint line suggests soft tissue
Limitation of motion - Reduced range of motion (both active and passive)
Bony swelling - Marginal osteophytes and bone remodelling
- Seen often in small joints (eg. finger interphalangeal, first metatarsophalangeal) and large joints (eg. knee)
Joint deformity - Sign of advanced damage
- Seen as squaring and subluxation of thumb base (first CMC)
Instability - Buckling common with knee OA
- Described as apprehension and lack of confidence to weight-bear
Classic findings of generalized OA:
- Heberden’s nodes (posterolateral swellings of DIP joints)
- Bouchard’s nodes (posterolateral swellings of PIP joints)
- Involvement of thumb bases
Joint distribution
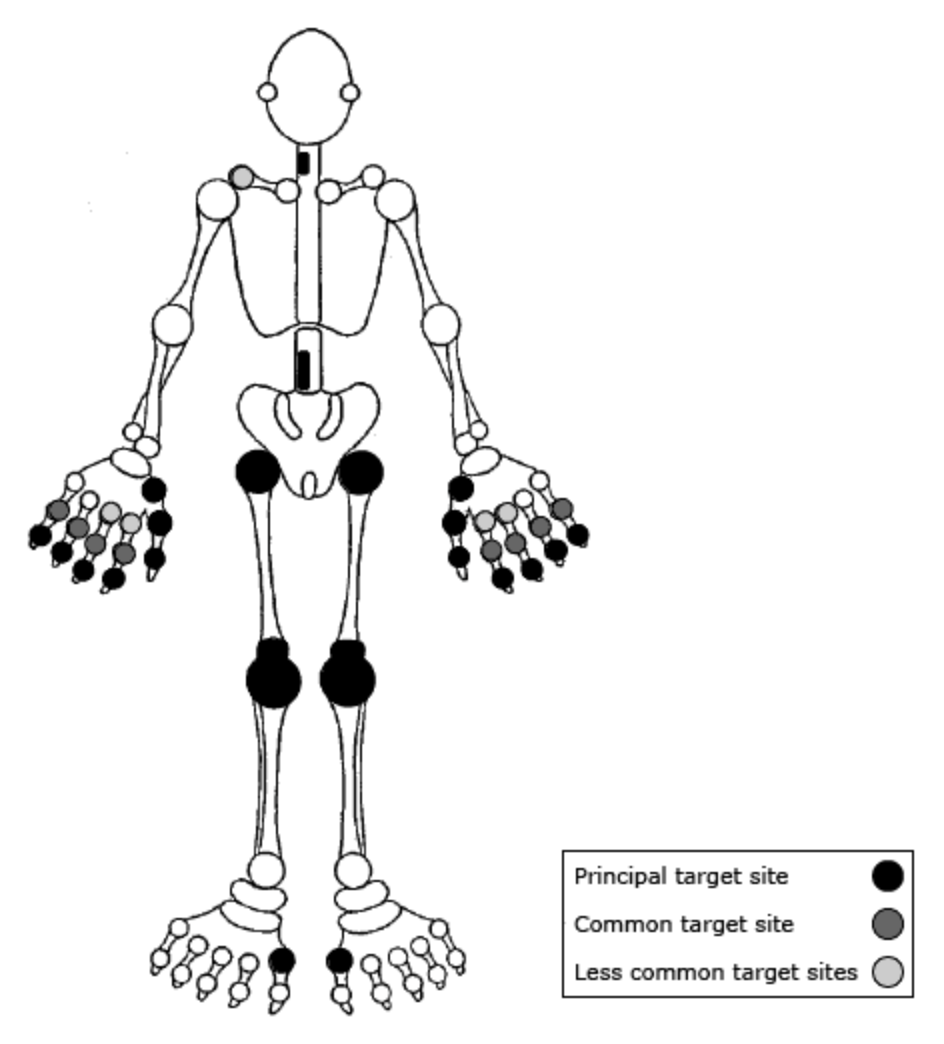
OA generally affects the knees, hips, DIPs, PIPs, first CMC, first MTP, and the facet joints of the lower cervical and lower lumbar spine.
The elbow and shoulder joints may be affected with occupation that involve overuse of upper extremities.
Joint involvement is more often unilateral but can also be bilateral.
History & Physical Exam
History and physical should find symptoms are consistent with OA. Additionally, the progression of the condition should be elicited:
- Symptom trajectory is gradual and progressive
- Presence and severity of flare-ups
- Unilateral nature
Diagnosis
Criteria
Diagnosis of osteoarthritis is made clinically based on the presence of typical symptoms and signs in the at-risk age group.
Peripheral join OA can be diagnosed if the following are present:
- Persistent usage-related joint pain in one or a few joints
- Age ≥45 years
- Morning stiffness ≤30 minutes
Work-up
While imaging is not routine, it can be used when there is ambiguity with the diagnosis (eg. if the patient age is young) or if assessment of severity is needed (eg. for arthroplasty).
Radiography can generally detect characteristic features of OA and measure joint space narrowing as a surrogate measure of cartilage loss. While symptoms do not necessarily correlate to severity of structural changes, the Kellgren and Lawrence OA grading system can be used:
- Grade 0: no joint space narrowing or osteophytes
- Grade 1: doubtful joint space narrowing with possible osteophytes
- Grade 2: Definite osteophytes and possible joint space narrowing (mild OA)
- Grade 3: Moderate osteophytes, definite joint space narrowing, some sclerosis, possible bone-end deformity (moderate OA)
- Grade 4: Large osteophytes, marked joint space narrowing, severe sclerosis, definite bone-end deformity (severe OA)
In some circumstances, MRI can be used for ruling out OA in causes where another diagnosis may be more likely (eg. meniscal tear). Ultrasound may also be used to evaluation of synovial inflammation, effusion, and osteophytosis, especially for hand and knee joints.
Synovial fluid analysis may be used if there is suspicion of crystalline arthopathy (eg. osteoarthritis with calcium pyrophosphate deposition, gout). Consider if morning stiffness is markedly longer and there are more signs of synovitis.
Differential
Osteoarthritis can generally be distinguished easily from other conditions. Similar diagnoses include:
- Rheumatoid arthritis - RA is DIP sparing; for thumb PIP instead of CMC; longer morning stiffness; inflammatory factors greater
- Psoriatic arthritis - DIP targeting but often just one finger with nail changes
- Crystalline arthritis - urate or CPP crystals in synovial fluid
- Hemochromatosis - targets MCP joints and wrists
- Infectious arthritis - inflammatory signs with day to day progression
- Other soft tissue abnormalities
Red Flags / Complications
Complications are related to the symptoms of OA such as pain, decreased ROM, and difficulties ambulating.
Other possible complications include radiculopathies.
Red flags include more emergent conditions such as infectious arthritis which can lead to sepsis.
Management
The goal of management are to minimize pain, optimize function, and reduce joint damage.
Lifestyle / Social
Non-pharmacologic therapy should be done prior to or in conjunction with medication. These generally target modifiable risk factors that contribute to pain.
- Weight management and exercise
- Braces and foot orthoses
- Use of assistive devices
Exercise in particular have been show to be comparable to NSAIDs in terms of effect on pain. Body weight loss has also been shown to reduce pain significantly especially in overweight or obese patients.
Misalignment can also be targeted with knee braces and walking aids and splits can be used for the thumb.
Pharmacological / Interventional
Pharmacological therapy should be used for symptomatic patients during periods when symptoms are present. These interventions are not disease-modifying and thus should not be used unnecessarily.
The specific therapy is selected based on effectiveness and contraindications.
- Topical NSAIDs
- Oral NSAIDs (lowest effective dose); for patients with comorbidities use cox-2 selective or nonselective plus PPI
- Duloxetine if NSAIDs are contraindicated (eg. GI bleed)
- Topical capsaicin
Intra-articular glucocorticoid injections are typically not routine due to the short duration of effect and possible negative effects on hyaline cartilage.
Acetaminophen is also not first-line as it has negligible effect on pain. Opioids are also not used apart from short-term severe or disabling symptoms that other therapies are unable to improve.
Surgical treatment consist primarily of total joint replacement. This is generally effective for patients with advanced knee and hip OA when other therapies fail to provide pain relief.