creation date: 2025-09-29 16:37
tags: Pathologies
Hyponatremia
Background
Definitions
Hyponatremia refers to an decrease of sodium relative to the water content of the body. The relevance of water content is due to sodium (and its anions) making up most of the effective osmoles in the extracellular fluid.
As such, serum sodium represents the water content of the body more so than the sodium levels and thus the approach to etiology, evaluation, and treatment revolves around water. In this case, hyponatremia reflects a relative excess of water.
Tonicity refers to the activity of solutes (in most cases, sodium) that do not easily cross cell membrane. As water can freely move across membranes, tonicity effectively dictates water movement, cell volume, and volume status.
- Hypertonicity refers to a high plasma sodium concentration
- Hypotonicity refers to a low plasma sodium concentration
Etiology
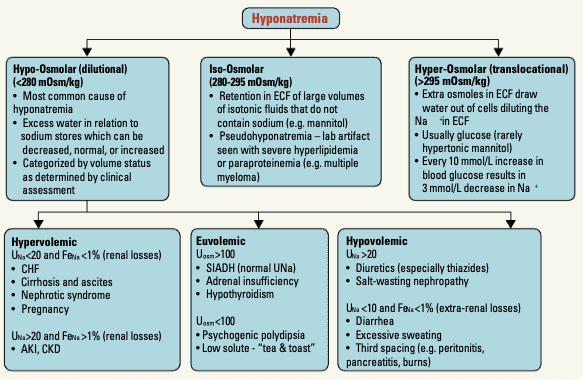
Causes of hypoosmolar hyponatremia is typically classified by the volume status of the extracellular fluid.
Hypovolemic hyponatremia (TBW decreases less than sodium decrease)
- Gastrointestinal fluid loss (eg. diarrhea, vomiting)
- Third spacing of fluid (eg. pancreatitis, SBO)
- Diuretics (especially thiazide which allows for some retention of water)
- Osmotic diuresis
- Salt-wasting nephropathies
- Cerebral salt-wasting syndrome (eg. increased BNP)
- Mineralocorticoid deficiency
Hypervolemic hyponatremia (TBW increases greater than sodium increase)
- Renal causes (eg. AKI, CKD, nephrotic syndrome)
- Extrarenal (eg. CHF, cirrhosis)
- Iatrogenic
Euvolemic hyponatremia (TBW increases with stable sodium)
- Syndrome of inappropriate antidiuretic hormone (SIADH)
- CNS injuries
- Medications (eg. SSRIs)
- Addison’s disease (adrenal insufficiency - causes low cortisol which results unopposed ADH)
- Hypothyroidism
- High fluid intake (eg. due to primary polydipsia)
- Beer / tea-and-toast diet - results in low electrolyte due to poor solute intake
- Iatrogenic
- Medications (eg. vasopressin analogs, thiazide diuretics, NSAIDs)
Pathogenesis
Normal plasma sodium concentration is maintained by thirst stimulation, arginine vasopressin secretion, and sodium processing in the kidneys. To maintain a consistent plasma osmolality, water intake should be equal to water excretion.
The water retention can result in a number of manifestations relating to the accumulation of fluid in spaces. Examples include cerebral edema, in which water shifts from the plasma and CSF into the brain, which can result in neurologic dysfunction.
Clinical Presentation
Signs & Symptoms
Acute hyponatremia manifests as symptoms of cerebral overhydration. These include:
- Nausea and malaise
- Headache, lethargy, obtundation
- Seizures, coma, respiratory arrest
In chronic hyponatremia, cerebral adaptations such as increasing interstitial hydraulic pressure and removal of brain cell solutes, reduce symptom burden. This can be asymptomatic or nonspecific symptoms such as:
- Fatigue
- Nausea and vomiting
- Dizziness
- Confusion
History & Physical Exam
History should elucidate possible etiology. Important to include are:
- History of pulmonary and CNS disorders
- Medications
- Social history including substance use (notably: beer intake or use of MDM or ecstasy)
- Recent treatment with mannitol, glycerol, IV Ig
- Recent surgery utilizing large volume of hypotonic fluid
Physical examination includes assessment of volume status and neurologic symptoms.
Risk factors
Diagnosis
Criteria
Hyponatremia is commonly defined as serum sodium below 135 mmol/L.
The exact type can be determined based on plasma osmolality:
- Hypotonic (plasma osmolality <275 mOsm/kg) - most common
- Isotonic (plasma osmolality 275-290 mOsm/kg)
- Hypertonic (plasma osmolality >290 mOsm/kg)
Severity is classified as:
- Mild: 130-134 mmol/L
- Moderate: 120-129 mmol/L
- Severe: <120 mmol/L
Work-up
The workup should exclude pseudohyponatremia which may be present in cases of hyperproteinemia (eg. multiple myeloma) or hyperlipidemia.
Common tests ordered initially include:
- Electrolytes
- Creatinine
- Glucose
Underlying disease may also be elucidated with:
- CBC
- LFTs
- Serum calcium
- TSH and AM cortisol
- Urine sodium and chloride and other urine tests
Serum osmolality is not a required test but can be ordered if hypertonic (eg. hyperglycemia) or isotonic (eg. multiple myloma) hyponatremia is suspected.
Urine osmolality can also confirm renal or extrarenal etiology.
Differential
Pseudohyponatremia may show hyponatremia on labs when sodium and water status are normal. Other differentials include the various underlying etiology.
Red Flags / Complications
While many effects of cerebral edema can be reversed on treatment, irreversible neurological damage is possible.
Management
Mild / moderate and asymptomatic
Patients with mild condition can generally be managed on an outpatient basis. In many cases, sodium will auto-correct, especially if the etiology is benign (eg. excessive water intake following marathon).
Severe / symptomatic
In severe (serum sodium <120 mmol/L) or symptomatic patients, treatment should be in hospital settings. The goal of inpatient treatment are to:
- Prevent further decline
- Decreased ICP if at risk of brain herniation
- Symptom management
- Avoid excessive correction
Acute hyponatremia
Typically, the urgency of correction is due to symptoms such as seizures. Treatment is:
- 100 mL bolus of 3% saline
- Up to two additional 100 mL boluses over 30 minutes
Chronic hyponatremia
In patients with severe symptoms, sodium repletion is necessary to alieviate symptoms:
- 100 mL bolus of 3% saline
- Up to two additional 100 mL boluses
In cases of mild to moderate symptoms with severe hyponatremia, treatment:
- 3% saline at 0.25 mL/kg/hr
- With or without desmopressin
In cases of mild to moderate symptoms with moderate hyponatremia, treatment of underlying cause is typically sufficient in correcting sodium.
Instead of 3% saline, normal saline may also be sufficient, and may be superior as there is lower risk of adverse events.
Rate of correction and monitoring
When using saline, it is crucial to maintain a safe rate of correction to avoid adverse effects. The goal is to raise serum sodium by 4-6 mmol/L in 24 hours with a maximum rate of 8 mmol/L in 24 hours. It is better to err on the side of slower correction.
Electrolytes should be repeated q3-4h at minimum for normal saline, and q1h for 3% saline.
Fluid restriction to below level of urine output (more out than in) is also indicated for symptomatic or severe hyponatremia in edematous states (eg. CHF or cirrhosis), SIADH, advanced kidney impairment, and primary polydipsia. Ingestion of salt should also be restricted.