creation date: 2025-06-25 22:22
tags: Pathologies
Atrial Fibrillation
Background
Definitions
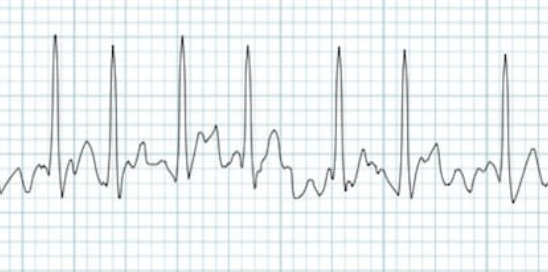
Atrial fibrillation (Afib) is a common cardiac arrhythmia. Afib is associated with an irregularly irregular ventricular rhythm and absence of distinct P waves.
Afib can be classified based on duration and length of episodes:
- Paroxysmal afib: terminates spontaneously or with intervention within seven days of onset
- Persistent afib: fails to self-terminate within seven days. Episodes often require pharmacologic or electrical cardioversion to restore sinus rhythm.
- Long-standing persistent afib: afib that has lasted for more than 12 months
- Permanent afib: persistent afib in which a decision has been made to no longer pursue rhythm control.
Afib typically progresses from paroxysmal to persistent states but this is not always the case.
Etiology and Pathogenesis
Afib shares a strong association with other cardiovascular diseases. Any condition that results in inflammation, stress, damage, or ischemia can alter the anatomy and electrophysiology of the atrial myocardium resulting in developing afib. These conditions are listed as risk factors.
The source of atrial fibrillation signals typically arises surrounding the pulmonary veins.
Reversible causes of afib include (PIRATE):
- Pulmonary disease / Pulmonary embolism
- Infections / Ischemia
- Remodelling of atria from cardiac disease / Rheumatic heart disease
- Alcohol / Anemia / Age
- Thyrotoxicosis
- Electrolyte abnormalities (K/Mg)
- Sepsis / Sleep apnea / Stress response
Premature atrial complexes (PACs) are often the trigger for paroxysmal afib for patients with normal or near-normal hearts.
In cases of valvular afib, the most common cause is mitral stenosis. This results in the dilation of the atria which changes the electrical circuitry.
Clinical Presentation
Signs & Symptoms
Symptoms are often broad and nonspecific. Afib may present with or without associated symptoms. Typical accompanying symptoms include:
- Palpitations
- Tachycardia
- Fatigue
- Weakness
- Dizziness
- Lightheadedness
- Reduced exercise capacity
- Increased urination
- Mild dyspnea
Severe symptoms may also be present which includes:
- Dyspnea at rest
- Angina
- Presyncope or rarely syncope
- Symptoms of stroke or other systemic embolic event
- Symptoms of heart failure
History & Physical Exam
Asymptomatic screening of patients is not routine.
Discovery of afib may occur during routine examination especially when associated symptoms are mentioned, incidentally during ECG, or during treatment of downstream complications such as stroke or other thromboembolism.
History should involve aspects of associated symptoms as well as presence of any associated conditions such as cardiovascular disease.
Afib can be palpated as an irregularly irregular pulse. The irregularity may also be heard on auscultation.
Risk factors
As mentioned previously, a number of conditions can lead to the development of afib. Some examples are:
- Advanced age
- Congenital heart disease
- Underlying heart disease - valvular disease, coronary artery disease, structural heart disease, atrial ischemia
- Increased alcohol consumption
- Hypertension - systemic or pulmonary
- Endocrine disorders - diabetes, pheochromocytoma, and hyperthyroidism
- Genetic factors
- Neurologic disorders - subarachnoid hemorrhage or stroke
- Hemodynamic stress - mitral or tricuspid valve disease, left ventricular dysfunction, pulmonary embolism
- Obstructive sleep apnea
- Inflammation - myocarditis and pericarditis
Diagnosis
Criteria
Diagnosis can be made using a 12-lead ECG. Findings include:
- Irregularly irregular rhythm
- No P waves
- Absence of an isoelectric baseline
- Variable ventricular rate
- QRS complexes usually <120ms, unless pre-existing conduction pathology
- Fibrillatory waves may be present which can be fine (amplitude < 0.5mm) or coarse (amplitude > 0.5mm)
If the afib is intermittent, ambulatory cardiac monitoring (eg. Holter monitor) can be used. It can also aid in correlating symptoms to the arrhythmia.
Work-up
With clinical suspicion of afib, the 12-lead ECG should be obtained.
An transthoracic echocardiogram should be done even if physical exam is normal. This is to evaluate:
- Size of right and left atria
- Size and systolic function of the right and left ventricle
- Detect possible valvular heart disease, LVH, diastolic dysfunction, and pericardial disease
- Assess peak right ventricular and right atrial pressures
- Presence of thrombus (low sensitivity)
A transesophageal echocardiogram is often used to check for thrombus prior to initiating rhythm control. A transesophageal view can better visualize the left atrial appendage which is where most thrombus will be.
Additional cardiac testing (eg. stress test) may be indicated if there are signs of ischemic heart disease.
Laboratory testing should be completed for CBC, serum electrolytes, and renal function assessment. Troponin is not indicated unless acute ischemia is suspected.
Differential
- Sinus rhythm with premature atrial complexes (which gives impression of irregularity)
- Atrial flutter - would be regular ventricular contraction
- Atrial tachycardia
- Multifocal atrial tachycardia
- WPW syndrome
- Atrioventricular nodal reentry tachycardia
Red Flags / Complications
The major complication of afib is the formation of thrombus. The rhythm irregularity causes heart blood flow to be turbulent and increases the likelihood of thrombus formation and systemic emboli, resulting in a stroke.
Management
Indication for emergency / in-patient
Emergency room visit is indicated for patients with:
- Hemodynamic instability and/or shock
- Suspected or confirmed myocardial ischemia/infarction
- Suspected or confirmed heart failure
- Evidence of pre-excitation on ECG (eg. WPW syndrome)
- Extreme, uncontrolled tachycardia
- Severe symptoms with urgent need for rate/rhythm control
- Hypotension for which afib is suspected to be causal or contributory
Patients should be hospitalized if:
- An ablation of an accessory pathway is being considered
- Severe bradycardia or prolonged pauses
- Treatment of an underlying cause of afib
- Management needed for heart failure or hypotension after control of rhythm or rate
- Initiation of antiarrhythmic drug therapy requires hospitalizaion (due to patient or drug characteristics)
- Difficult to control ventricular rates with evidence of heart conditions
Initial management
Anticoagulation
Antithrombotic therapy should be considered to prevent systemic embolization. Evaluation of risk for incidental stroke can be done using the CHA2DS2-VASc score. Anticoagulation is indicated for a score ≥2 in males and ≥3 in females. This is weighed against the HAS-BLED score for bleeding risk.
Hemodynamically unstable
In hemodynamically unstable patient with signs of hypotension, altered mental status, or heart failure, ventricular rate control should be attempted. This may lead to spontaneous reversion to sinus rhythm.
If patient is normotensive:
- IV diltiazem with initial bolus of 0.25 mg/kg
- IV metoprolol, esmolol, or verapamil if diltiazem does not slow heart rate
If hypotensive:
- If vasopressor not used, metoprolol tartrate 25mg PO q6h and up-titrated
- If on vasopressor or symptomatic hypotension, consider electrical cardioversion
Emergency cardioversion should be done if patient remains unstable. Cardioversion can be done pharmacologically or electrically and decision should be made based on factors such as patient preference, comorbidities, stability, and efficacy.
- Synchronized cardioversion
- Pharmacological cardioversion is typically by flecainide or propafenone
Hemodynamically stable
Afib can be managed in the outpatient setting. Evaluate whether rate needs to be controlled or if cardioversion is necessary. This is discussed below as part of long-term management.
Catheter ablation
In some cases, ablation may be an appropriate treatment for rhythm control. It is typically indicated for symptomatic patients with paroxysmal or persistent afib who are refractory or intolerant to antiarrhythmic drugs but still stable enough for procedure.
- Pulmonary vein isolation
- AV node ablation
Valvular surgery
In cases of valvular afib, treatment of underlying condition (eg. valve replacement) is indicated to resolve afib.
Long-term management
Lifestyle changes
Modifications that can reduce afib recurrence and/or symptom burden include:
- Alcohol reduction
- Weight loss and physical activity
Anticoagulation
Based on assessment done on stroke risk, the decision to undergo anticoagulation should be made. A direct oral anticoagulant (DOAC) is preferred over warfarin due to the ease of use.
Direct Oral Anticoagulants are discussed in detail separately. Some options are:
- Apixaban 5 mg PO BID
- Dabigatran 150mg PO BID
In patients with with mechanical valves, warfarin is used. Warfarin is bound to albumin and may need to be adjusted in cases of cirrhosis, nephrotic syndrome, or malnutrition. Dosing is titrated based on regular INR measurements.
Dosing may need to be adjusted based on renal impairment.
Rate control
Slowing of ventricular rate is often initiated during initial management. The target rate is typically 85 bpm in a patient without heart disease. In asymptomatic individuals with permanent afib, a more lenient rate goal of <110 bpm can be considered.
This can be accomplished with an oral cardioselective beta blocker, rate-slowing nondihydropyridine calcium channel blocker, or digoxin.
- Diltiazem or verapamil
- Atenolol, metoprolol, timolol, pindolol, or nadolol
- Digoxin is usually not preferred due to narrow therapeutic window but may be used with afib and heart failure due to its effect on improving cardiac output
- A combination of a beta blocker and a calcium channel blocker may be considered if monotherapy is inadequate
Rhythm control
Should rate control be inadequate for symptom management, rhythm control should be considered. For patients at high risk of cardiovascular disease, this may also be preferred.
Prior to starting an antiarrhythmic, patient should be rate controlled and sinus rhythm should be restored (eg. with cardioversion).
Several antiarrhythmics can be chosen but most commonly used are:
- Amiodarone 100-200mg PO once daily (lower dose for older or low BMI patients)
- Other options include dofetilide, flecainide, propafenone, and sotalol
Propafenone can also be carried around as a “pill-in-pocket” approach to paroxysmal afib for spontaneous onset.
References
Tools / Guidelines
MDCalc - Atrial fibrillation stroke risk calculator
MDCalc - bleeding risk calculator