creation date: 2025-11-20 20:34
tags: Pathologies
Alcohol-Associated Liver Disease
Background
Definitions
Alcohol-associated liver disease (ALD) refers to a spectrum of disorders relating to the consumption of alcohol.
The three histologic stages of ALD consists of:
- Alcoholic steatosis
- Alcoholic hepatitis
- Alcoholic cirrhosis
Etiology and Pathogenesis
The pathology of ALD arises through the consumption and metabolism of ethanol.
Liver steatosis
Ethanol is metabolized via several pathways and is described as follows:
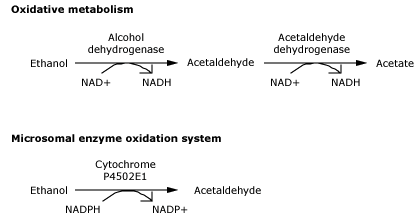
While the liver can tolerate mild alcohol consumption, increased in consumption can lead to metabolic disorders.
As metabolism increases, the production of NADH increases as a result of the metabolism pathway. The shifting of NAD+ and NADH metabolism results in the formation of glycerol phosphate which combine with fatty acids to produce triglycerides, which accumulate in the liver.
Alcohol consumption also decreases lipid oxidation (lipolysis) leading to fat accumulation.
Genetic determinants also increase the fat accumulation within the liver.
Liver injury and hepatitis
In some patients, liver steatosis may develop to steatohepatitis. A number of factors contribute to this transition such as immunologic defects (activation of innate immunity amplifying inflammation).
The inflammation involves:
- Neutrophil infiltration and activation
- Endotoxins and cytokines
Additionally, impaired regeneration due to chronic ethanol ingestion and changes to gut microbiome may be implicated in liver disease.
Ethanol also has hepatotoxic characteristics (mitochondria toxin) which can independently cause damage to the liver, particularly in zone 3, which is furthest from the artery, increasing its risk to hypoxia.
Inflammation results in injury and ballooning of the hepatocytes. Ongoing liver injury leads to irreversible damage, referred to as cirrhosis.
Clinical Presentation
Signs & Symptoms
Presentation of ALD vary with disease severity.
Most patients are asymptomatic or have nonspecific symptoms such as fatigue. Alcoholic hepatitis often presents with fever, jaundice, and RUQ tenderness.
In the most extreme of spectrum, decompensated cirrhosis can present with jaundice, peripheral edema, abdominal distension from ascites, hematemesis, or melena.
Physical findings may include hepatomegaly and findings of cirrhosis.
Associated features may include:
- AST elevated but <8x ULN
- ALT elevated but <5x ULN
- AST/ALT >1 (often >2)
- GGT often elevated
- Anemia (macrocytosis)
Other laboratory findings include:
- Thrombocytopenia
- Leukopenia
- Elevated INR
- Hyponatremia
- Elevated creatinine (if hepatorenal syndrome)
History & Physical Exam
Initial evaluation may include:
- Description of symptoms
- Existing medical conditions
- Medication use (incl. herbal and OTC)
- Riak factors for other causes of livery disease (eg. exposure to viral hepatitis)
- Family history of liver conditions
- Alcohol consumption
Physical should include:
- Assessment for hepatomegaly
- Stigmata for chronic liver disease jaundice, ascites, splenomegaly, gynecomastia)
- Extra-hepatic manifestations of alcohol use disorder (skeletal muscle wasting, cardiomyopathy, neuropathies)
Risk factors
Diagnosis
Criteria
The diagnosis of ALD is made through clinical, laboratory, and liver imaging in a patient with a history of harmful alcohol use in the absence of other primary etiologies.
Diagnostic liver biopsy and histology can also be used if diagnosis is uncertain.
Work-up
In patients with suspected ALD, the following studies are done to assess liver function and comorbid conditions:
- ALT, AST, ALP, GGT
- Total bilirubin and serum albumin
- PTT/INR
- CBC with platelets
- Fasting blood glucose and A1C
- Lipid panel
Additional tests for alternative causes include:
- Hepatitis B screening (surface antigen, surface antibody, total core antibody)
- Anti-hep C virus antibody
- Iron panel
- Antimitochondrial antibody for primary biliary cholangitis
- IgG and antibodies for autoimmune hepatitis
- Ceryuloplasmin (in patients <50 with neurocognitive symptoms) for Wilson disease
- Alpha-1 antitrypsin level for AAT deficiency
- Anti-tissue tTG-IgA for celiac disease
Staging of disease
The goal of staging is to determine the severity of fibrosis. Biopsy is sufficient for evaluation for patients who underwent liver biopsy for diagnosis. Otherwise:
- Vibration-controlled transient elastography: ultrasound-based measurements of liver stiffness (stiffness correlated to degree of fibrosis)
- Acoustic radiation force impulse (ultrasound-based)
- Magnetic resonance elastography
Differential
Other conditions that cause liver steatosis include:
- Metabolic dysfunction-associated steatotic liver disease
- Chronic hepatitis C infection
- Parenteral nutrition
- Drug-induced liver disease
- Wilson disease
- Other genetic diseases
Red Flags / Complications
Management
General Measures
The cornerstone of ALD management is abstinence from alcohol. Consider referring patients for treatment of alcohol use disorder. In early stages (pre-cirrhosis), cessation will generally return liver back to normal.
Nutritional deficiencies should be assessed and addressed with goals of:
- Total daily energy intake of 35 kcal/kg of body weight
- Total daily protein intake of 1.2-1.5 g/kg of bodyweight
Consider enteral nutrition if requirements are not met with oral ingestion.
Immunization for hepatitis A and B should be given to patients without serologic immunity.
Continued monitoring for signs and symptoms of disease progression, including laboratory studies, should be obtained every 3 months.