creation date: 2026-04-28 18:51
tags: Assessments
Dermatology Lesions
Background
Evaluation of skin lesions should consider elements of the history including:
- Presence of infectious symptoms
- Onset and duration
- Past medical history
- Precipitating events
- Changes/evolution
Lesions
Benign
Acrochordons (Skin Tags)

Clinical Findings
- Soft, flesh-coloured pedunculated papules
- Located in skin folds (neck, axillae, groin, eyelids)
- Range from 1mm to >1cm
- Non-tender, easily moveable
- Multiple lesions common
Pathophysiology
- Benign fibrovascular polyps from superficial dermis
- Friction at skin folds + hyperinsulinemia stimulates fibroblast/keratinocyte proliferation
- Strongly associated with obesity and metabolic syndrome
Diagnosis/Treatment
- Clinical diagnosis
- Snip excision, electrocautery, or cryotherapy if symptomatic
- Consider metabolic risk review given obesity and diabetes.
Differential Diagnosis
- Intradermal nevus
- Neurofibroma
- Small seborrheic keratosis
Benign Melanocytic Nevus (Compound/Congenital-Pattern)

Clinical Findings
- Well-defined, symmetric, uniformly pigmented papule
- Tan to brown color, smooth or slightly raised
- Stable size and appearance over years
- Clear borders without irregularity
- Usually <6mm
Pathophysiology
- Benign proliferation of melanocytes at the dermoepidermal junction and/or dermis
- Stable lesion due to oncogene-induced arrests
Diagnosis/Treatment
- ABCDE review and dermoscopy
- Photograph and monitor if stable and symmetric
- Excisional biopsy if evolution, asymmetry, irregular pigment, or bleeding
Differential Diagnosis
- Dysplastic nevus
- Melanoma
- Seborrheic keratosis
Blue Nevus

Clinical Findings
- Well-defined blue-gray to blue-black papule or nodule
- Smooth surface, usually <1cm
- Most common on dorsal hands, feet, scalp, sacrum
- Stable, present since childhood or young adulthood
- Firm on palpation
Pathophysiology
- Dermal melanocyte proliferation creates blue-gray color via the Tyndall effect
- Melanocytes in dermis due to arrest during neural crest migration to epidermis
Diagnosis/Treatment
- Dermoscopic assessment and baseline photo if longstanding and stable
- Excisional biopsy if new change, growth, bleeding, or diagnostic uncertainty
Differential Diagnosis
- Melanoma
- Combined nevus
- Pigmented dermatofibroma
Cherry Angiomas

Clinical Findings
- Bright red, dome-shaped papules 1–5mm
- Blanch completely with pressure
- Most common on trunk
- Increase in number with age
- Bleed readily if traumatized
Pathophysiology
- Benign proliferation of superficial capillaries that increases with age due to increased VEGF expression
Diagnosis/Treatment
- Clinical diagnosis
- Reassure if typical
- Electrocautery or laser if bleeding or cosmetically bothersome
Differential Diagnosis
- Pyogenic granuloma
- Angiokeratoma
- Amelanotic melanoma
Dermatofibroma

Clinical Findings
- Firm, slightly raised brownish papule
- Positive dimple sign (puckering on lateral compression)
- Hyperpigmented center, paler periphery
- Most common on lower legs
- Slightly tender on palpation
Pathophysiology
- Benign fibrohistiocytic reaction, often after minor trauma or insect bite, producing a firm dermal nodule with dimpling
- Dimpling due to tethering of epidermis to underlying fibrous nodule
Diagnosis/Treatment
- Clinical diagnosis including dimple sign
- Reassure if classic and stable
- Biopsy if enlarging, atypical, painful, or diagnostically uncertain
Differential Diagnosis
- Epidermoid cyst
- Dermatofibrosarcoma protuberans
- Nodular melanoma
Epidermoid Cyst

Clinical Findings
- Smooth, dome-shaped skin-colored nodule
- Central punctum (key feature)
- Cheesy, malodorous contents if expressed
- Tender and red if inflamed/ruptured
- Mobile unless previously ruptured
Pathophysiology
- Keratin-filled cyst from follicular infundibulum obstruction or epidermal implantation
- Rupture triggers inflammation and malodorous drainage
Diagnosis/Treatment
- Clinical diagnosis
- If acutely inflamed, consider I&D or intralesional steroid
- Definitive treatment is complete excision of cyst wall once quiescent
Differential Diagnosis
- Sebaceous cyst (oily, yellow sebum due to oil glands)
- Pilar cyst
- Abscess
- Lipoma
Infantile Hemangioma

Clinical Findings
- Absent or faint at birth, appears weeks 1–4 of life
- Bright red, strawberry-like papule or plaque
- Rapid growth phase over first year
- Gradual spontaneous involution over years
- Superficial (bright red) vs. deep (bluish, compressible) subtypes
Pathophysiology
- Postnatal endothelial proliferation with a rapid growth phase followed by gradual involution over years
Diagnosis/Treatment
- Assess for ulceration, visual obstruction, airway risk, and high-risk site involvement
- Observe if uncomplicated
- Oral propranolol is first-line if function-threatening or ulcerated
Differential Diagnosis
- Congenital hemangioma
- Vascular malformation
- Pyogenic granuloma
Keloid

Clinical Findings
- Raised, firm, rubbery scar that extends beyond wound margins
- Progressive growth over time (distinguishes from hypertrophic scar)
- Pruritic and sometimes painful
- Hyperpigmented, shiny surface
- Predisposition in darker skin types; earlobes, sternum, shoulders common sites
Pathophysiology
- Abnormal wound healing with excess collagen deposition extending beyond the original injury margins
Diagnosis/Treatment
- Clinical diagnosis
- First-line: intralesional triamcinolone ± silicone/pressure therapy
- Avoid simple excision alone due to high recurrence risk
Differential Diagnosis
- Hypertrophic scar
- Dermatofibroma
- Epidermoid cyst
Keratoacanthoma

Clinical Findings
- Rapid growth over 6-8 weeks
- Dome-shaped, flesh-colored nodule with central keratin-filled crater
- Symmetrical “volcano-like” architecture
- Sun-exposed skin in elderly, fair-skinned patients
- May spontaneously involute over months
Pathophysiology
- Rapidly proliferating crateriform squamoproliferative lesion on sun-damaged skin, regarded as a well-differentiated SCC variant
Diagnosis/Treatment
- Excisional biopsy/complete removal (indistinguishable from SCC clinically)
- Histology guides further margins or surveillance
Differential Diagnosis
- Cutaneous squamous cell carcinoma
- Verruca
- Nodular BCC
Keratosis Pilaris

Clinical Findings
- Multiple small (1–2mm) rough follicular papules
- Keratinous plug within follicle
- Mild perifollicular erythema
- Posterior upper arms and anterolateral thighs (classic sites)
- Worsens in winter and low humidity; non-pruritic
Pathophysiology
- Follicular keratin plugging causes rough small papules on extensor surfaces, often worse with dry weather
Diagnosis/Treatment
- Reassure; benign chronic condition
- Moisturizers plus keratolytics (urea, lactic acid, or salicylic acid)
- Gentle skin care and avoid over-scrubbing
Differential Diagnosis
- Folliculitis
- Lichen spinulosus
- Phrynoderma
Lipoma

Clinical Findings
- Soft (consistency similar to tip of nose), doughy, compressible subcutaneous mass
- Mobile and “slips” under finger
- Not attached to overlying skin
- Typically non-tender
- Slow growing, usually 1–5cm
Pathophysiology
- Benign tumour of mature adipocytes in subcutaneous tissue
Diagnosis/Treatment
- Clinical diagnosis
- Ultrasound if deep, fixed, large, painful, or rapidly enlarging
- Excision only if symptomatic or uncertain
Differential Diagnosis
- Epidermoid cyst
- Angiolipoma
- Liposarcoma
Seborrheic Keratosis
Clinical Findings
- “Stuck-on” verrucous/waxy papules or plaques
- Variable pigmentation (tan to dark brown)
- Rough, pasted-on appearance
- Horn cysts on dermoscopy
- Common on trunk, face, extremities in older adults
Pathophysiology
- Benign clonal proliferation of epidermal keratinocytes
- Somatic mutations accumulates with aging
- No UV-dependent mechanism or malignant potential
Diagnosis/Treatment
- Clinical diagnosis with dermoscopy
- Reassure if classic
- Cryotherapy/curettage if irritated or cosmetically bothersome; biopsy if atypical or rapidly changing
Differential Diagnosis
- Solar lentigines
- Pigmented BCC
- Melanoma
Pre-malignant / Malignant
Actinic Keratosis

Clinical Findings
- Rough, sandpaper-textured papules/patches
- Erythematous base with adherent scale
- On chronically sun-exposed skin (scalp, face, dorsal hands, forearms)
- Background photoaging and solar damage
- Tender when palpated
Pathophysiology
- Chronic UV damage causes mutation and atypia of epidermal keratinocytes
- Premalignant lesion on the SCC spectrum
- Progression risk rises with immunosuppression
Diagnosis/Treatment
- Full skin exam for field cancerization
- Cryotherapy for discrete lesions or field therapy with 5-FU/imiquimod if extensive
- Biopsy any thick, tender, or indurated lesion
Differential Diagnosis
- SCC in situ/Bowen disease
- Superficial BCC
- Seborrheic dermatitis
Basal Cell Carcinoma (Nodular Type)

Clinical Findings
- Pearly, translucent papule with rolled borders
- Surface telangiectasia
- Easy bleeding with minor trauma
- Slow-growing over months to years
- Almost exclusively on sun-exposed skin (face, nose, ears)
Pathophysiology
- UV-driven malignancy of basal keratinocytes with hedgehog-pathway dysregulation causes pearly telangiectatic papules that bleed easily
Diagnosis/Treatment
- Shave or punch biopsy for confirmation
- Definitive treatment is excision or Mohs surgery given nasal location
- Sun protection and skin cancer surveillance.
Differential Diagnosis
- Fibrous papule
- Sebaceous hyperplasia
- Amelanotic melanoma
Melanoma

Clinical Findings
- ABCDE criteria: Asymmetry, irregular Border, multiple colours (tan/brown/black/pink), Diameter >6mm, Evolution
- Change in a pre-existing mole
- Variegated pigmentation (shades of brown to black with possible pink/white areas)
- May ulcerate or bleed spontaneously
- Most common on back (men) and legs (women)
Pathophysiology
- Malignant melanocytic proliferation with radial and/or vertical growth produces ABCDE features including colour variegation and irregular borders
Diagnosis/Treatment
- Urgent excisional biopsy with narrow margins
- Stage by Breslow depth after pathology
- Wide local excision ± sentinel node biopsy depending on depth
Differential Diagnosis
- Dysplastic nevus
- Pigmented seborrheic keratosis
- Pigmented BCC
Squamous Cell Carcinoma

Clinical Findings
- Firm, indurated hyperkeratotic nodule or plaque
- Ulcerated or crusted surface
- Erythematous base, non-healing
- Sun-exposed areas (ears, lower lip, dorsal hands, scalp in bald patients)
- Rapid growth, tenderness, and induration suggest invasive disease
Pathophysiology
- UV-damaged atypical keratinocytes invade the dermis
- Immunosuppression increases risk and aggressiveness.
Diagnosis/Treatment
- Urgent biopsy (high-risk), rapidly growing nasal lesion
- Likely excision/Mohs after histologic confirmation
- Examine for nodal disease if advanced features present
Differential Diagnosis
- Keratoacanthoma
- Hypertrophic actinic keratosis
- Basal cell carcinoma
Inflammatory / Autoimmune
Allergic Contact Dermatitis (Urushiol/Poison Ivy Exposure)

Clinical Findings
- Linear streaks of vesicles/bullae (hallmark of plant contact)
- Intensely pruritic erythematous plaques
- Distribution follows contact pattern
- Delayed onset 24–72 hours after exposure
- Can spread by scratching/residual urushiol (oil from poison ivy)
Pathophysiology
- Type IV delayed hypersensitivity after plant exposure produces intensely pruritic vesicular dermatitis
Diagnosis/Treatment
- Clinical diagnosis based on exposure pattern
- Wash skin/clothing
- High-potency topical steroid if localized
- Oral prednisone taper if severe, widespread, or facial/genital involvement
Differential Diagnosis
- Irritant contact dermatitis
- Phytophotodermatitis
- Arthropod bite reaction
Alopecia Areata

Clinical Findings
- Smooth, circular/oval patches of complete hair loss
- No scarring, scaling, or inflammation of scalp
- “Exclamation mark” hairs at periphery (tapered proximally)
- Nail pitting in ~10–20% of cases
- Sudden onset, often associated with stress
Pathophysiology
- Autoimmune T-cell attack on anagen hair follicles causes smooth round patches of nonscarring hair loss
Diagnosis/Treatment
- Clinical diagnosis with dermoscopy if available
- Intralesional steroid for limited disease; potent topical steroid if preferred
- Review associated autoimmune history
Differential Diagnosis
- Tinea capitis
- Trichotillomania
- Traction alopecia
Atopic Dermatitis

Clinical Findings
- Flexural distribution (antecubital/popliteal fossae, wrists, ankles)
- Intense pruritus (“itch that rashes”)
- Xerosis and lichenification in chronic disease
- Dennie-Morgan lines (infraorbital folds)
- Personal or family history of atopy (asthma, allergic rhinitis)
Pathophysiology
- Skin barrier dysfunction (often filaggrin-related) plus Th2-skewed inflammation causes chronic pruritic flexural eczema
Diagnosis/Treatment
- Daily emollients and trigger avoidance
- Topical corticosteroid for flares
- Consider calcineurin inhibitor or escalation if recurrent/moderate-severe
Differential Diagnosis
- Allergic contact dermatitis
- Scabies
- Fungal infection
- Psoriasis
Bullous Pemphigoid

Clinical Findings
- Large, tense bullae on urticarial or erythematous base
- Bullae do not rupture easily (subepidermal, tense)
- Extremities and flexures most commonly involved
- Prodrome of intense pruritus weeks before blisters
- Elderly patients; minimal mucosal involvement
Pathophysiology
- IgG autoantibodies against BP180/BP230 at the basement membrane produce subepidermal tense bullae, often after a prodromal pruritic phase
Diagnosis/Treatment
- Biopsy (H&E stain + perilesional DIF)
- High-potency topical steroid if localized; systemic steroid or steroid-sparing therapy if extensive
Differential Diagnosis
- Bullous drug eruption
- Linear IgA bullous dermatosis
- Pemphigus vulgaris
Dyshidrotic Eczema (Pompholyx)
Clinical Findings
- Deep-seated, intensely pruritic “tapioca-like” vesicles
- Lateral aspects of fingers, palms, and soles
- Vesicles do not rupture easily (thick overlying skin)
- Followed by scaling, fissuring, and peeling as lesions resolve
- Cyclic recurrences, often triggered by stress or heat
Pathophysiology
- Recurrent vesicular hand-foot dermatitis linked to sweat, stress, atopy, or contact allergy
- Stress causes autonomic activation and sweating which activates inflammatory cascade
- Palmar/plantar stratum corneum results in vesicles deep in the epidermis and thus do not rupture easily
Diagnosis/Treatment
- High-potency topical steroid and frequent emollients
- Hand protection and trigger control
- KOH if unilateral hand/foot to rule out dermatophyte
Differential Diagnosis
- Tinea manuum/pedis
- Scabies
- Herpetic whitlow
Erosive Vulvovaginal Lichen Planus

Clinical Findings
- Painful erosive lesions on vulvar/vaginal mucosa
- White, lacy reticulated borders (Wickham striae) adjacent to erosions
- Glazed erythema and friability
- Dyspareunia and vaginal discharge common
- Scarring and architectural distortion in chronic disease
Pathophysiology
- T-cell-mediated autoimmune on basal keratinocytes of mucosal epithelium
- Keratinocyte apoptosis and basal cell degeneration
- 1-2% risk of SCC transformation
Diagnosis/Treatment
- Vulvar biopsy if any uncertainty or cancer concern
- High-potency topical corticosteroid is first-line
- Gynecology/dermatology follow-up for symptom control and SCC surveillance
Differential Diagnosis
- Lichen sclerosus
- Chronic candidiasis
- Vulvar intraepithelial neoplasia/SCC
Nummular Eczema

Clinical Findings
- Coin-shaped (nummular), well-demarcated eczematous plaques
- Vesicles, crusting, and oozing within lesions
- Intensely pruritic, often worse at night
- Extremities and trunk common sites
- Chronic dry skin background; worsens in winter
Pathophysiology
- Xerosis and epidermal barrier dysfunction lead to coin-shaped, intensely pruritic eczematous plaques
Diagnosis/Treatment
- Emollients plus medium/high-potency topical steroid
- KOH if annular appearance raises diagnostic doubt
- Reduce irritants and winter xerosis
Differential Diagnosis
- Tinea corporis
- Plaque psoriasis
- Allergic contact dermatitis
Pemphigus Vulgaris

Clinical Findings
- Flaccid, easily ruptured bullae on normal-appearing skin
- Positive Nikolsky sign (shearing normal skin causes erosion)
- Extensive painful erosions
- Oral mucosa almost always involved (often first site)
- Weight loss due to painful eating
Pathophysiology
- Autoantibodies to desmoglein 3 (and possibly Dsg1) cause intraepidermal acantholysis, flaccid bullae, and painful mucosal erosions
Diagnosis/Treatment
- Urgent biopsy and DIF
- Systemic corticosteroids plus rituximab or other steroid-sparing therapy
- Address hydration, nutrition, and infection risk
Differential Diagnosis
- Mucous membrane pemphigoid
- Paraneoplastic pemphigus
- Bullous pemphigoid
Perioral Dermatitis

Clinical Findings
- Small erythematous papules and pustules clustered around the mouth
- Characteristic sparing of a 2-5mm zone at the vermilion border
- May extend to perinasal and periorbital areas
- History of topical steroid use (often initially improves, then worsens)
- Predominantly in young women
Pathophysiology
- Topical corticosteroids impair barrier and alter microbiome
- Barrier disruption results in innate immune activation
- Similar mechanism to rosacea
Diagnosis/Treatment
- Stop topical steroid and avoid heavy facial products
- Topical metronidazole/erythromycin or pimecrolimus; oral doxycycline if extensive
- Expect temporary rebound after steroid withdrawal
Differential Diagnosis
- Acne vulgaris
- Rosacea
- Allergic/irritant contact dermatitis
Plaque Psoriasis

Clinical Findings
- Well-demarcated erythematous plaques with thick silvery-white scale
- Predilection for extensor surfaces (elbows, knees), scalp, lower back
- Auspitz sign (pinpoint bleeding when scale removed)
- Koebner phenomenon (lesions at trauma sites)
- Nail pitting and onycholysis common
Pathophysiology
- IL-23/Th17-driven inflammation due to dysregulated innate immunity
- keratinocyte hyperproliferation with accelerated turnover, causing sharply demarcated erythematous plaques with silvery scale
Diagnosis/Treatment
- Confirm clinically; assess nails and joints for psoriatic arthritis
- Topical steroid plus vitamin D analog if limited
- Systemic therapy if extensive or joint disease present
Differential Diagnosis
- Chronic eczema
- Tinea corporis
- Seborrheic dermatitis
Rosacea (Papulopustular/Erythematotelangiectatic)

Clinical Findings
- Central facial erythema (cheeks, nose, forehead, chin)
- Telangiectasia and persistent flushing
- Papules and pustules without comedones
- Triggered by heat, spicy food, alcohol, sunlight
- Rhinophyma (sebaceous hyperplasia of nose) in severe/chronic cases
Pathophysiology
- Overexpression of genes result in pro-inflammatory cytokines
- Neurovascular hyperreactivity causes flushing and angiogenesis
- Demodex mites (naturally occurring skin mites) amplify immune response
- Th1/Th17 infllammation results in papulopustular formation
Diagnosis/Treatment
- Trigger avoidance and gentle skin care
- Topical metronidazole, azelaic acid, or ivermectin first-line
- Oral doxycycline if more inflammatory
Differential Diagnosis
- Acne vulgaris
- Perioral dermatitis
- Cutaneous lupus erythematosus
Seborrheic Dermatitis

Clinical Findings
- Greasy, yellowish-white scale with erythema
- Predilection for nasolabial folds, eyebrows, scalp, external ear canals, chest
- Chronic relapsing course
- Worsens with stress, fatigue, neurological disease
- Dandruff is a mild scalp form
Pathophysiology
- Malassezia yeast metabolizes sebum triglycerides (in sebum rich areas such as face and scalp)
- Free fatty acids from metabolized TGs disrupt skin barrier
- Disrupted skin barrier allows for inflammatory activation
Diagnosis/Treatment
- Ketoconazole shampoo/cream
- Short course low-potency steroid or calcineurin inhibitor for flares
- Maintenance antifungal for recurrent disease.
Differential Diagnosis
- Psoriasis
- Atopic dermatitis
- Tinea faciei/capitis
Urticaria

Clinical Findings
- Transient (<24h) pruritic, erythematous wheals with pale center
- Lesions migrate and change shape
- Surrounding erythematous flare
- Dermographism may be present
- Angioedema of lips/eyes/tongue possible
Pathophysiology
- Type 1 hypersensitivity (IgE mediated) mast-cell degranulation releases histamine, prostaglandins, leukotrienes
- Increased vascular permeability causes wheal with or without flare
Diagnosis/Treatment
- Non-sedating H1 antihistamine; up-dose if needed
- Assess for angioedema or anaphylaxis
- Short steroid burst only if severe and not responsive
Differential Diagnosis
- Urticarial vasculitis
- Drug eruption
- Contact dermatitis
Vitiligo

Clinical Findings
- Chalk-white, well-demarcated, completely depigmented patches
- Accentuated under Wood lamp (bright white fluorescence)
- Perioral, periocular, acral, and genital predilection
- Progresses over time
- Associated with other autoimmune diseases (thyroid, T1DM)
Pathophysiology
- Autoimmune destruction of melanocytes causes sharply demarcated depigmented patches
Diagnosis/Treatment
- Clinical diagnosis
- Wood lamp can confirm
- Screen for associated autoimmune conditions
- Topical steroid/calcineurin/JAK inhibitor for limited disease; nbUVB if extensive
Differential Diagnosis
- Tinea versicolor
- Post-inflammatory hypopigmentation
- Pityriasis alba
Infectious
Cellulitis

Clinical Findings
- Unilateral expanding erythema, warmth, swelling, and tenderness
- Poorly demarcated borders (distinguishes from erysipelas)
- Entry wound often visible (abrasion, ulcer, tinea pedis)
- Systemic signs (fever, malaise) possible
- Most common on lower extremities
Pathophysiology
- Acute bacterial infection of dermis/subcutis, usually streptococcal or staphylococcal, entering through a skin break
Diagnosis/Treatment
- Assess for abscess, systemic toxicity, and necrotizing infection
- Start oral anti-streptococcal/anti-staphylococcal antibiotic and elevate the leg
- Mark borders and reassess if diabetic
Differential Diagnosis
- Deep venous thrombosis
- Stasis dermatitis
- Contact dermatitis
Erythema Migrans (Early Lyme Disease)

Clinical Findings
- Expanding annular erythematous rash (>5cm) with or without central clearing
- “Bull’s eye” pattern: central clearing with outer expanding ring
- Appears 3–30 days after tick bite
- Located at or near bite site (typically thigh, groin, axilla)
- Recent tick exposure or camping/outdoor activity history
Pathophysiology
- Local cutaneous infection with Borrelia burgdorferi after Ixodes tick exposure produces an expanding annular erythematous lesion
- Expansion due to spirochetal spread through dermis
- Partial central clearance due to immune response
- Without treatment can disseminate to other systems causing complications
Diagnosis/Treatment
- Treat clinically without waiting for serology if presentation is classic
- Doxycycline in adults; amoxicillin as an alternative
- Review for neurologic, cardiac, or joint symptoms
Differential Diagnosis
- Tinea corporis
- Cellulitis
- Southern tick-associated rash illness (STARI)
Herpes Labialis (HSV-1 Reactivation)

Clinical Findings
- Prodrome of tingling, burning, or itching 12–24h before eruption
- Grouped vesicles on erythematous base at vermilion border
- Rapid progression: vesicles to pustules to crust
- Heals over 7–10 days
- Recurs at same site with subsequent triggers (UV, stress, fever)
Pathophysiology
- HSV reactivates from latency in the trigeminal ganglion, causing prodromal tingling followed by grouped painful vesicles
Diagnosis/Treatment
- Start oral antiviral early (within prodrome/first 48 hours)
- Supportive care and avoid direct contact during active lesions
- Consider suppressive therapy if recurrent
Differential Diagnosis
- Impetigo
- Aphthous lesion near vermilion
- Contact cheilitis
Herpes Zoster

Clinical Findings
- Painful prodrome (burning, tingling) preceding rash by days
- Unilateral dermatomal grouped vesicles on erythematous base
- Does not cross the midline
- Most common thoracic dermatomes (T3–L3)
- Risk of post-herpetic neuralgia, especially in elderly/immunocompromised
Pathophysiology
- Reactivation of latent VZV in a dorsal root ganglion causes painful unilateral dermatomal vesicular eruption
- Risk increased by immunosuppression (age related, chemotherapy)
Diagnosis/Treatment
- Start valacyclovir/acyclovir promptly with analgesia
- Monitor closely given active chemotherapy
- Urgent review if disseminated or ophthalmic/neurologic symptoms develop
Differential Diagnosis
- HSV infection
- Allergic contact dermatitis
- Zosteriform metastatic eruption
Measles (Rubeola)


Clinical Findings
- Prodrome: 3 Cs (Cough, Coryza, Conjunctivitis) + high fever
- Koplik spots: white/gray dots on buccal mucosa (pathognomonic, appear 1-2 days before rash)
- Maculopapular rash starts at hairline/face and spreads cephalocaudally
- Lesions may become confluent
- Unvaccinated child in endemic or outbreak setting
Pathophysiology
- Paramyxovirus enters respiratory system via epithelial cells resulting in primary viremia
- Secondary viremia seeds skin, respiratory tract, CNS
- Viral antigens present in dermal vessels causes CD4 T cell immune response, producing rash
Diagnosis/Treatment
- Immediate airborne isolation and public health notification
- Confirm with PCR/serology
- Supportive care plus vitamin A per pediatric guidance
Differential Diagnosis
- Rubella
- Roseola
- Adenoviral/other viral exanthem
Molluscum Contagiosum

Clinical Findings
- Multiple 2–5mm dome-shaped flesh-coloured papules
- Central umbilication (pathognomonic)
- White cheesy core can be expressed
- Clusters in moist/intertriginous areas
- Surrounding eczematous reaction (“molluscum dermatitis”) common
Pathophysiology
- Poxvirus infection of epidermal keratinocytes
- Inhibits MHC-1 expression and blocks apoptosis for local immune evasion leading to delayed immune recognition (and thus resolution)
Diagnosis/Treatment
- Usually clinical diagnosis and watchful waiting
- Treat if spreading with cantharidin, curettage, or cryotherapy
- Manage associated eczema to reduce scratching
Differential Diagnosis
- Verruca vulgaris
- Milia
- Folliculitis
Nonbullous Impetigo

Clinical Findings
- Honey-colored/golden crusted erosions (pathognomonic)
- Perioral and perinasal distribution most common
- Fragile vesicles/pustules rupture quickly leaving crusts
- Mildly pruritic, non-tender
- Spreads readily by scratching/contact
Pathophysiology
- Superficial epidermal infection (S. aureus or group A strep) causes
- Superficial blister rupture results in honey-coloured crusts
- Spreads by contact and autoinuoculation
Diagnosis/Treatment
- Clinical diagnosis
- Topical mupirocin if limited; oral antibiotic if extensive
- Hygiene and nail trimming to reduce spread
Differential Diagnosis
- HSV infection
- Periorificial dermatitis
- Excoriated eczema
Pityriasis Rosea

Clinical Findings
- Herald patch: solitary large (2–10cm) oval erythematous patch with collarette scale, precedes rash by 1–2 weeks
- Diffuse smaller oval patches following skin cleavage lines (“Christmas tree” pattern on back)
- Spares face, palms, and soles
- Mild pruritus
- Self-resolving in 6–12 weeks
Pathophysiology
- Likely post-viral inflammatory eruption (HHV-6/7)
- Viral antigen triggers Th1 response
- Herald patch from initial replication site
- Subsequent lesions follow cleavage lines via viremic spread
Diagnosis/Treatment
- Clinical diagnosis
- KOH or RPR if atypical
- Reassure; topical steroid or antihistamine for itch
Differential Diagnosis
- Tinea corporis
- Guttate psoriasis
- Secondary syphilis
Plantar Warts (Verruca Plantaris)

Clinical Findings
- Hyperkeratotic papules on weight-bearing surfaces
- Black dots (thrombosed capillaries) - pathognomonic
- Disruption of normal skin lines
- Pain with direct pressure and pinching (distinguishes from callus)
- May coalesce into mosaic warts
Pathophysiology
- HPV infection of plantar keratinocytes causes hyperkeratotic papules with thrombosed capillaries visible as black dots
Diagnosis/Treatment
- Clinical diagnosis, sometimes aided by paring
- Topical salicylic acid or cryotherapy
- Counsel on autoinoculation and foot hygiene
Differential Diagnosis
- Corn/callus
- Pitted keratolysis
- Foreign body granuloma
Roseola Infantum (Exanthem Subitum)

Clinical Findings
- High fever (39-40 deg C) lasting 3–5 days in a well-appearing child
- Abrupt defervescence followed immediately by rash
- Rose-pink maculopapular rash on trunk, spreading to extremities
- Rash non-pruritic and fades within days
- Most common in children 6-24 months
Pathophysiology
- Primary HHV-6/7 infection after maternal antibody wanes (~6 months of age)
- Virus replicates in CD4 T cells causing systemic viremia and high fever
- As viremia clears (and thus fever), immune response on skin results in transient maculopapular rash
Diagnosis/Treatment
- Clinical diagnosis and supportive care
- No specific treatment if well appearing
- Review hydration and seizure history if fever was very high
Differential Diagnosis
- Measles
- Rubella
- Enteroviral exanthem
Scabies

Clinical Findings
- Intensely pruritic, worse at night
- Linear burrows in finger webs, wrists, waistline, axillae, genitalia
- Erythematous papules and vesicles
- Spares head and neck in immunocompetent adults
- Close contacts with similar symptoms (highly contagious)
Pathophysiology
- Sarcoptes scabiei infestation triggers delayed hypersensitivity, causing nocturnal itch, papules, and burrows in classic sites
- Initial infestation: 4-6 weeks sensitization before itch starts
- Re-infestation: 24-48 hrs before itch
- Type IV hypersensitivity to mite antigens, eggs, and feces
Diagnosis/Treatment
- Treat patient and close contacts with permethrin 5% or oral ivermectin
- Wash/dry bedding and clothing on hot cycle
- Topical steroid/antihistamine for post-treatment itch
Differential Diagnosis
- Atopic dermatitis
- Papular urticaria
- Contact dermatitis
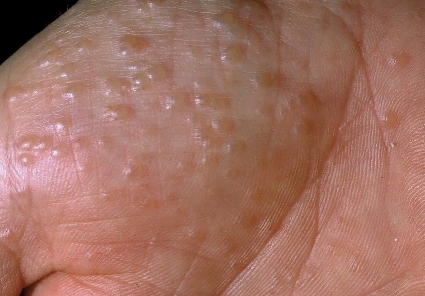
Secondary Syphilis

Clinical Findings
- Copper-coloured papulosquamous rash involving palms and soles (classic and distinctive)
- Generalized non-tender lymphadenopathy
- Constitutional symptoms (malaise, low-grade fever, sore throat)
- Condylomata lata (flat moist lesions in intertriginous areas)
- Painless chancre history 6–8 weeks prior
Pathophysiology
- Hematogenous dissemination of Treponema pallidum after the primary chancre stage causes systemic symptoms and a palm/sole papulosquamous eruption
Diagnosis/Treatment
- RPR/VDRL plus treponemal confirmation
- Treat with benzathine penicillin G (discuss desensitization or alternative if severe penicillin allergy)
- Notify public health and treat contacts
Differential Diagnosis
- Pityriasis rosea
- Viral exanthem/drug eruption
- Psoriasis
Tinea Capitis

Clinical Findings
- Scaly patches with partial alopecia
- Broken “black dot” hairs at follicle openings
- Cervical lymphadenopathy common
- Kerion: boggy, indurated, pustular inflammatory mass
- Predominantly in prepubertal children; contagious within households
Pathophysiology
- Dermatophyte invade hair shaft
- Spores weaken hair causing black dot breakage
- Kerion due to exaggerated hyper IV hypersensitivity to antigens resulting in boggy inflammatory mass (pustular)
Diagnosis/Treatment
- Confirm with fungal culture/KOH
- Systemic terbinafine or griseofulvin - topical therapy alone is inadequate (fungi penetrate below topical drug depth)
- Antifungal shampoo for household contacts
Differential Diagnosis
- Alopecia areata
- Seborrheic dermatitis
- Traction alopecia
Tinea Corporis

Clinical Findings
- Annular erythematous plaque with central clearing
- Active, scaly, slightly raised advancing border
- Pruritic
- Single or multiple lesions
- KOH demonstrates branching hyphae
Pathophysiology
- Dermatophyte infection of the stratum corneum causes an annular plaque with central clearing and a scaly advancing edge
- Central clearing caused by neutrophil immune clearance
Diagnosis/Treatment
- Confirm with KOH if uncertain
- Topical terbinafine or azole cream
- Avoid topical steroid monotherapy
Differential Diagnosis
- Nummular eczema
- Granuloma annulare
- Pityriasis rosea herald patch
Tinea Versicolor

Clinical Findings
- Multiple well-defined hypo- or hyperpigmented patches with fine scale
- Trunk, shoulders, and upper arms most common
- Scale accentuated by stretching skin
- KOH shows “spaghetti and meatballs” (short hyphae + round spores)
- Worsens in summer/heat; asymptomatic or mildly pruritic
Pathophysiology
- Malassezia convers to mycelial form in warm, humid conditions
- Produces azelaic acid which inhibits tyrosinase causing hypopigmentation
- Inflammatory response may result in hyperpigmentation in darker skin
Diagnosis/Treatment
- Clinical diagnosis; KOH can confirm “spaghetti and meatballs” pattern
- Selenium sulfide or topical ketoconazole first-line
- Explain that pigment normalization lags behind fungal clearance
Differential Diagnosis
- Vitiligo
- Pityriasis alba
- Post-inflammatory hypopigmentation
Varicella (Chickenpox)

Clinical Findings
- “Dewdrop on a rose petal” vesicles on erythematous base
- Lesions in multiple simultaneous stages (macule, papule, vesicle, crust)
- Centripetal distribution (face and trunk > extremities)
- Intensely pruritic
- Fever and malaise precede rash
Pathophysiology
- Primary VZV infection from respiratory droplets to upper respiratory lymph nodes
- Secondary viremia seeds skin causing keratinocyte infection and intraepidermal vesicle formation
Diagnosis/Treatment
- Clinical diagnosis and isolation
- Supportive care if otherwise healthy
- Consider oral acyclovir if early and high-risk or severe
Differential Diagnosis
- Disseminated HSV
- Eczema herpeticum
- Papular urticaria
Pigmentation Disorder
Solar Lentigines (sun spots)


Clinical Findings
- Flat, well-defined, uniformly brown macules
- 1–3cm on chronically sun-exposed areas (dorsal hands, face, forearms)
- No elevation or palpable texture
- Persistent (unlike freckles, do not fade in winter)
- Background of photoaging
Pathophysiology
- Chronic UV exposure increases melanocyte activity and melanin deposition, producing flat brown macules on sun-exposed skin
- Excess of melanin production persists even during winter (unlike freckles)
Diagnosis/Treatment
- Clinical/dermoscopic diagnosis
- Biopsy any irregular, very dark, or changing lesion
- Sun protection; optional topical lightening or laser for cosmesis
Differential Diagnosis
- Freckles/ephelides
- Lentigo maligna
- Flat seborrheic keratoses
Melasma

Clinical Findings
- Symmetric, irregular brown-gray hyperpigmented patches
- Cheeks, forehead, upper lip, and chin distribution
- Worsens with sun exposure
- Predominantly in women of reproductive age, darker skin types
- Associated with OCP use or pregnancy (“mask of pregnancy”)
Pathophysiology
- Estrogen/progesterone upregulate genes within melanocytes
- UV exposure and hormonal stimulation increase melanogenesis, producing symmetric facial hyperpigmentation
Diagnosis/Treatment
- Clinical diagnosis
- Strict photoprotection (tinted mineral sunscreen)
- Hydroquinone/triple-combination cream
- Reduce estrogen trigger if feasible
Differential Diagnosis
- Post-inflammatory hyperpigmentation
- Lichen planus pigmentosus
- Drug-induced hyperpigmentation
Other
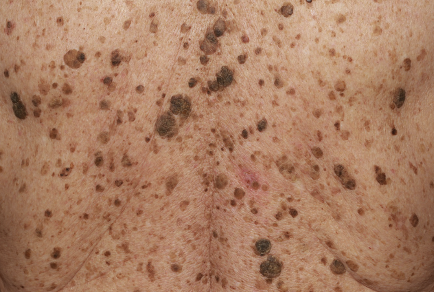
Neurofibromatosis Type 1 (NF1)

Clinical Findings
- ≥6 cafe-au-lait macules (>5mm prepubertal, >15mm postpubertal)
- Axillary or inguinal freckling (Crowe sign)
- Multiple soft, flesh-coloured neurofibromas
- Lisch nodules (iris hamartomas) on slit-lamp exam
- Autosomal dominant; diagnosis by NIH clinical criteria
Pathophysiology
- Loss-of-function of NF1 gene causes uncontrolled proliferation of neural crest-derived cells
- Disordered melanocyte development results in cafe-au-lait macules
Diagnosis/Treatment
- Confirm clinical criteria; genetics if uncertain
- Ophthalmology, BP monitoring, neurologic review, and hereditary counseling
- Remove symptomatic neurofibromas selectively
Differential Diagnosis
- Legius syndrome
- Schwannomatosis
- Multiple lipomas with incidental lentigines
Spider Angiomas

Clinical Findings
- Central red arteriole (“spider body”) with radiating thin capillaries
- Blanches with central point pressure, refills from centre outward
- Typically on face, neck, upper chest
- Multiple lesions in pregnancy or liver disease
- Resolves postpartum in most cases
Pathophysiology
- Elevated estrogen (pregnancy, liver disease, OCP use) upregulates VEGF and nitric oxide
- Arteriolar dilation and central arteriole dilates and feeds surrounding radially arranged capillaries
Diagnosis/Treatment
- Reassure if isolated and pregnancy-related (benign)
- No treatment needed unless bothersome; pulsed-dye laser is an option
- Broader workup only if numerous or atypical; suspicion of underlying disease
Differential Diagnosis
- Telangiectasia
- Cherry angioma
- Hereditary hemorrhagic telangiectasia lesions