creation date: 2026-04-21 22:48
tags: Assessments
Cardiac Auscultation
Background
Heart auscultation is an integral component of the cardiovascular exam.
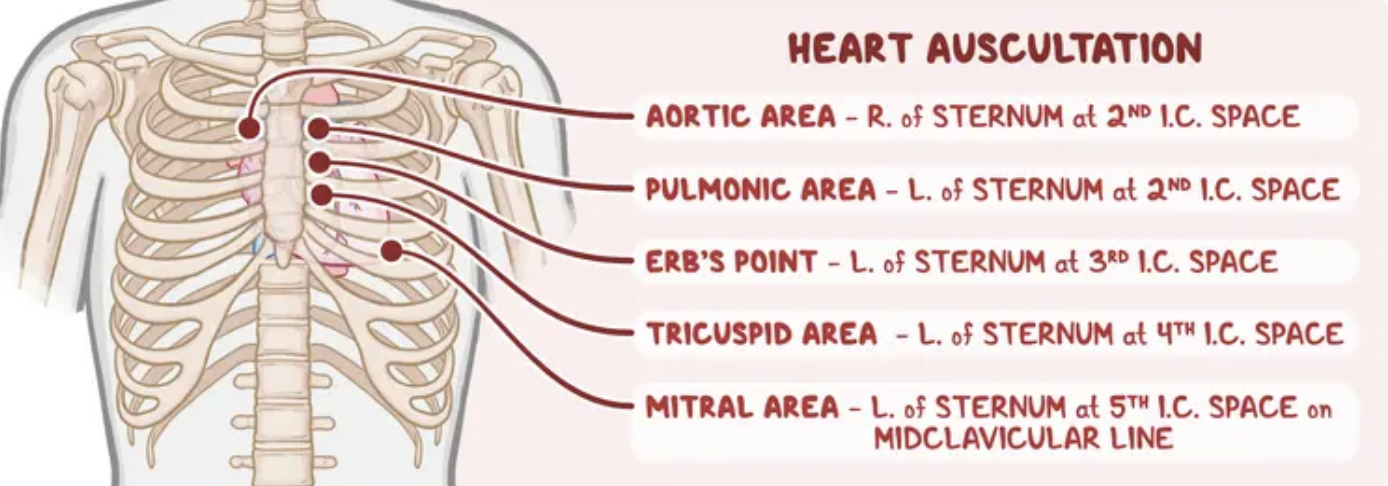
Each point is used to best auscultate their respective valves. Erb’s point is where S2 is best heard.
Physiological Heart Sounds
Heart Sounds
Normal heart sounds consist of the S1 and S2.
S1:
- Closing of the mitral and tricuspid valves
- Mitral precedes tricuspid by 0.04 s
- Onset of isovolumetric ventricular contraction (beginning of systole)
- Best heard at the mitral area
S2:
- Closing of aortic and pulmonic valves
- Aortic precedes pulmonic slightly (due to higher aortic pressures)
- Onset at end of systole
- Best heard at upper sternal borders
Other physiologically normal sounds include
Physiological S2 splitting:
- Occurs with young individuals
- On inspiration, increased venous return increases preload which delays the pulmonic valve closure
- Should not be present on expiration
S3:
- Occurs in early diastole (0.12-0.2s after S2)
- Corresponds to end of rapid ventricular filling
- Only physiological in children, young adults (≤40) and pregnant women
- Due to compliant ventricle and higher cardiac output
Pathological Heart Sounds
Extra Heart Sounds
S3:
- Pathological if adult aged >40
- Indicates volume overload (overfilled ventricle and poorly compliant)
- Causes include:
- Systolic heart failure
- Mitral regurgitation
- Dilated cardiomyopathy
- Hyperthyroidism (high-output state)
S4:
- Caused by forceful atrial contraction against stiff, non-compliant ventricle
- Causes include:
- Hypertension
- Left ventricular hypertrophy
- Aortic stenosis
- Hypertrophic cardiomyopathy
- Acute MI
Ejection sounds:
- High-pitched “click” heard in early systole
- Caused by sudden opening of abnormal valve
- Early ejection click - aortic or pulmonic stenosis
- Mid-systolic click - mitral valve prolapse
Murmurs
Murmurs are graded on a scale of I-VI:
- I - Barely audible, requires concentration
- II - Soft but easily heard
- III - Moderately loud, no thrill
- IV - Loud with palpable thrill
- V - Very loud, heard with stethoscope partially off chest
- VI - Audible without stethoscope
Systolic Murmurs
Ejection systolic (crescendo-decrescendo)
- Aortic stenosis: loudest at aortic area, radiates to carotids
- Causes: calcification, bicuspid valve, rheumatic disease
- Pulmonic stenosis: loudest at pulmonic area
- Causes: tetralogy of fallot
- Hypertrophic obstructive cardiomyopathy
- increases with Valsalva and standing (due to decreased preload), decreases with squatting
Pansystolic (holosystolic)
- Mitral regurgitation: loudest at mitral area/apex, radiates to axilla
- Causes: infective endocarditis, MI, rheumatic disease, cardiomyopathy
- Tricuspid regurgitation: loudest at tricuspid area, increases with inspiration
- Associated with: large JVP v-wave, hepatic pulsations, right-sided heart failure signs
- Ventricular septal defect: loud, harsh, at left sternal border
Late systolic
- Mitral valve prolapse: mid-systolic click, followed by late systolic murmur
Diastolic Murmurs
Early diastolic (decrescendo)
- Aortic regurgitation: aortic area, best heard when leading forward and expiration
- Associated with: collapsing pulse, hyperdynamic apex, wide pulse pressure
- Pulmonary regurgitation: high pitched at pulmonary area
- Associated with: pulmonary hypertension
Mid-diastolic (rumbling)
- Mitral stenosis: low-pitched rumble at mitral area with preceding opening snap, best heard when laying on left side
- Associated with: afib, malar flush, low-volume pulse, rheumatic origins
- Tricuspid stenosis: similar to mitral but tricuspid area, louder on inspiration
Continuous Murmurs
Heard throughout systole and diastole, crossing S2
Patent ductus arteriosus (PDA)
- Blood shunts from aorta to pulmonary artery continuously
- “Machinery murmur”, loudest at left infraclavicular area
Coarctation of the aorta
- Systolic component from turbulent aortic flow
- Diastolic component from associated aortic regurgitation
Arteriovenous fistula
- Continuous bruit over fistula site