creation date: 2025-08-01 02:33
tags: Anatomy & Physiology
Menstrual Cycle
Background
The menstrual cycle refers to the female cyclic change in preparation for ovulation and potential pregnancy. This begins with menarche (median age of 12.4) and ends with menopause (mean age of onset of 51).
By definition, the first day of heavy menstrual flow is considered day 1 of the cycle. Normal parameters are:
- Frequency between 24-38 days
- Duration ≤8 days
- Flow ≤80 mL per cycle
- Regularity variation ≤7 days (for age 18-25 or 42-45, difference of up to 9 days considered normal)
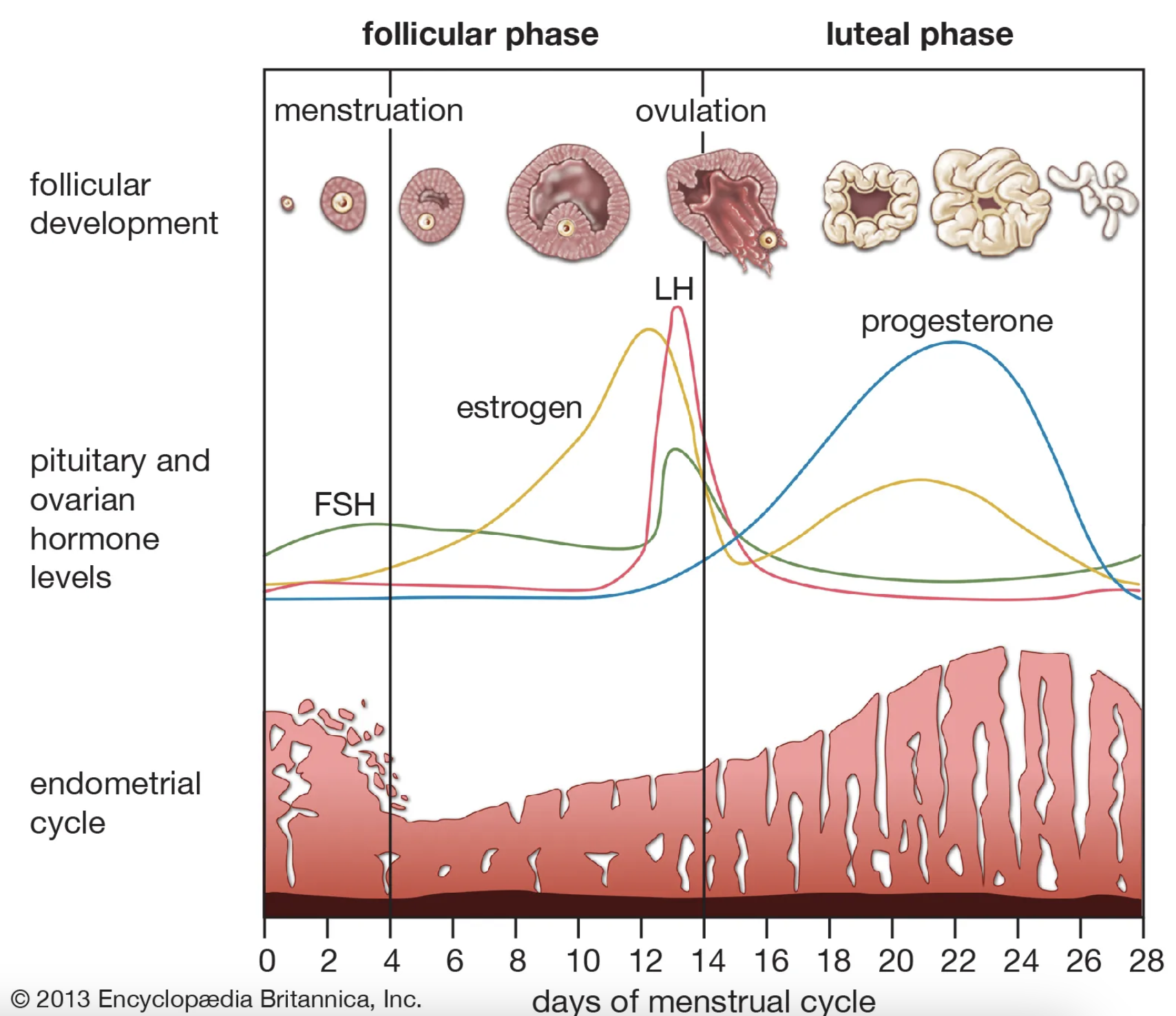
The menstrual cycle consist of 2 distinct cycles:
- Ovarian cycle, which consist of the follicular phase, ovulation, and luteal phase
- Endometrial cycle, which consist of the proliferative phase, secretory phase, and menstrual phase
Generally, the ovarian follicular phase corresponds to the endometrial menstrual and proliferative phases, while the ovarian luteal phase corresponds to the endometrial secretory phase.
The changes that occur throughout the menstrual cycle is summarized here:
Phases
Phase 1
Phase one consist of the ovarian follicular phase that occurs simultaneously to the endometrial menstrual phase and proliferative phase.
This phase can vary in duration but starts with menses and continues until ovulation.
Follicular Phase (Ovarian)
FSH level stimulates a cohort of primordial follicles to mature follicles which produce 17-β estradiol and inhibin B. The estradiol levels increases throughout the phase reaching its peak shortly before ovulation.
Around day 7, the negative feedback by estradiol and inhibin reduces FSH levels and the nondominant follicles degenerate. The lower FSH levels does not affect the dominant follicle due to increased FSH sensitivity.
The dominant follicle grows during this phase at a rate of 2 mm/day until it reaches 18-29 mm. LH receptors also develop in preparation for ovulation.
Menstrual Phase (Endometrial)
Follow the end of the previous cycle’s phase 2, a sudden decline in progesterone and estradiol levels results in an unsustainable endometrium. This, along with the release of prostaglandins which constrict the spiral arteries, results in the shedding of the endometrium.
Menstrual fluid contains blood, endometrial cells, vaginal secretions, and biochemical molecules such as proteolytic enzymes, cytokines, and products of fibrinolysis. Menstrual fluid typically does not contain clots unless the flow is very heavy.
Proliferative Phase (Endometrial)
After the endometrium finishes shedding, the proliferative phase begins in preparation for the next potential pregnancy. The estradiol produced by the the follicles stimulates the growth of the endometrial stroma and glands from the decidual basalis. The spiral arteries also increase in depth to supply the endometrium.
The endometrium typically grows between 8-12 mm and the cervical mucus also changes in elasticity and protein content by the end of the proliferative phase.
Ovulation
14 days before the onset of menses, ovulation typically occurs. As the estradiol levels increase past a threshold level near the end of the follicular phase, it transitions from providing negative feedback (and thus suppressing FSH and LH secretion) to positive feedback at the anterior pituitary. Hypotheses for this mechanisms suggests the elevated estradiol causes:
- Increased GnRH receptors, enhancing sensitivity
- Prevention of breakdown of GnRH
- Suppression of GnRH during follicular phase causing increased sensitivity at end of the phase
The positive feedback of the estradiol stimulates a sudden surge in LH secretion (10-fold increase) and small surge in FSH. This surge results in the rupture of the follicle and release of the oocyte approximately 36-44 hours after the LH surge.
In conjunction with the oocyte release, the cervix continues to change, resulting in a watery cervical mucus. Estradiol levels decrease after ovulation.
Phase 2
Phase 2 consist of the luteal and secretory phases. This phase begins with ovulation and ends when menstrual bleeding starts. Unlike phase 1, this phase is typically consistent within an individual, lasting around 14 days.
Luteal Phase (Ovarian)
Following the release of the oocyte, the LH and FSH causes the remaining part of the follicle to develop into the corpus luteum. This structure produces progesterone and subsequently estrogen.
In the case where fertilization occurs, the ovum releases human chorionic gonadotropin (hCG) which continues to stimulate the corpus luteum, maintaining progesterone production.
Without a fertilized ovum however, the progesterone and estrogen enacts negative feedback at the pituitary gland. This slows LH release and causing the corpus luteum to atrophy, degenerating it into a corpus albicans which no longer produce hormones. Progesterone and estrogen levels therefore decreases releasing GnRH from its negative feedback, reseting the hormones for the next cycle.
Secretory Phase (Endometrial)
With the increasing levels of progesterone, the endometrium matures in preparation for potential fertilized ovum implantation. This includes:
- Development of complex glands
- Increased glycogen accumulation for energy
- Increased surface area of the spiral arteries
- Thickening and decreased elasticity of the cervical mucus (more difficult for sperm to pass through)
- Increased basal body temperature
The endometrium also continues to thicken more from the estrogen.